


1. Background / Introduction
Acute pancreatitis (AP) in the recent years showed increasing frequency. There is better diagnostic performance, but there is also more wide knowledge about clinical appearance of different severity. The global incidence has been observed with very variable range, characterized by territorial differences. In the developed countries there is the trend in rising over the past several decades: 5-80 cases per years per 100.000 adults; e.g. in USA 40/100.000, in Finland 73/100.000, in Germany 17/100.000, in Australia 17/100.000, in Italy 35/100.000. On the contrary there is lower incidence in the developing nations [1-4]. AP is an inflammatory disease that can develop oedematous or necrotic forms. Edematous pancreatitis is the most frequent ( 80% of cases), the necrotic one is less frequent (20% of cases).
1.1 Etiology
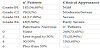
The etiology of AP is extremely variable and better characterized although regional and demographic variations exist. Several etiological factors can be listed. Biliary lithiasis and excessive alcohol consumption are the most frequent causes (80%). The remaining 20% constitutes a various group of causes [5]. The etiological factors can be summarized based on pathophysiology as genetic causes (hereditary pancreatitis), obstructive causes (gallstones, neoplasia, pancreas divisum), metabolic causes (alcohol, hyperlipidemia, hypercalcemia), drugs. Another subdivision criteria of etiological factors can be employed: common causes, uncommon, rare (Table 1).

In the AP there are also territorial variations of etiology. The very diversified territorial distribution of the various clinical and etiological forms of pancreatitis generated uncertainties. The etiological factors should be evaluated regarding geographical criteria; are in evidence for example the frequence differences between biliary and alcoholic etiology. The pancreatitis is a disease characterized by territorial and etiological differences based on life-style, habits, genetic factors, etc. Considering etiological factors by country there emerged evident differences concerning cholelithiasis and alcohol consumption.
The research has been performed; collecting data from various European countries, on etiological characteristics of the disease [6]. This research confirms different etiology prevalence related to country. Biliary etiology is more frequent in Italy and Greece; on the contrary is less frequent in Germany and France with difference statistically significant. The same study shows etiological differences related to age and gender: biliary etiology is more frequent in aged patients [6].
There is a evident prevalence of men vs women in pancreatitis with alcoholic etiology; more little prevalence in women for biliary etiology. The mean age is low for onset of alcoholic pancreatitis vs biliary etiology is in evidence that the alcohol is the most frequent etiological factor in the countries of the North Europe. The patients with the biliary etiology represent the oldest group of the patients. The different distribution of etiologies is not entirely clear but can be explained by the difference in alcohol consumption and incidence of cholelithiasis between north and south Europe.
We can estimate etiological differences lied on territorial distribution that are characteristic of AP and should be caused by life-style, habits, genetic factors. Moreover biliary etiology usually is related to acute forms, whereas the alcoholic underlies the chronic appearance.
The complex characteristcs of the disease, such as territorial differences of etiology, pathological features, clinical presentations and evolutions suggest some questions:
- The etiological and regional differences can explain the different clinical appearance and evolution?
- Alcoholic etiology may cause true AP that is with impairment of the general conditions over the abdominal pains?
- AP, also by biliary etiology, can develop the chronic pancreatitis?
- In summary there are connections between acute and chronic forms?
For all these questions the answers are object of deep discussions without stable and shared conclusions.
The first interesting question is: the etiological and regional distribution differences can explain the different clinical appearance and evolution? In the comparison between biliary and alcoholic pancreatitis, the most frequent etiologies, should be the first evaluation. Following the traditional scenario, the biliary etiology is related to AP, whereas the alcoholic underlies the chronic forms. The majority of other causes of pancreatitis is connected with acute forms. In other words we have to assess whether the alcoholic etiology may cause true acute pancreatitis with the impairment of the general conditions over the abdominal pains; or on the other hand if the AP can develop the chronic disease. The pathogenetic development of pancreatitis can clear up the connection between acute and chronic forms. AP is clinical manifestation of autodigestive process caused by premature activation of proteolytic pancreatic enzymes within the pancreas. The trypsin is firstly activated and then other proenzymes. The question is if the alcohol can cause the autodigestive phlogosis by enzymatic activation. There are several pathological actions of alcohol consumption reported in the literature. Alcohol causes increase of protein concentration in the pancreatic secretion with the formation of protein plugs which block the excretory ducts. The obstruction of pancreatic ductules starts the inflammatory process within the lumen of pancreatic ductules, that may progress to sclerosis, but without enzymatic digestive action. On the contrary the origin of the acute pancreatitis tends to be inside the acinar cells (enzymatic digestive action). Moreover pancreatic toxicity of the alcohol consumption is dose dependent and is necessary the prolonged chronic use. It’s in fact not demonstrated the alcohol acute toxicity. In summary alcoholic pancreatitis, chronic and its acute clinical presentation, are different clinical appearances of the same disease with same etiology and same pathology. Following the clinical experience we can report the acute onset of chronic pancreatitis with severe abdominal pains but without proteolytic necrotic parenchymal lesions and without impairment of general conditions. They were assumed other pathological effects of alcohol: reduction or increase of pression of Oddi sphincter with ductal pancreatic reflux of duodenal or biliary secretions. Other hypothesized alcohol effects should be the dicrease of the proteolytic anti-enzymes, effective in the pancreatic acini regarding the contrast of premature activated proteolytic pancreatic enzymes. Moreover the alcohol abuse should reduce the blood flow and oxygen perfusion in the pancreatic parenchyma. Finally has been also proposed the direct toxic action of alcohol on the acinar cells by increase and fusion of lisosom and zymogen granule that promote the intracellular activation of pancreatic enzymes. Parenchymal phlogosis follows with edema, hemorrhage, necrosis. This hypothesis shows the pathological picture very similar between the AP and acute onset of alcoholic pancreatitis [7,8,9].
Other causes less frequent of pancreatitis are post-procedural ERCP, trauma, drugs, infections, ductal obstruction such as in pancreas divisum, tumors, etc., hypercalcemia, hypertriglyceridemia, genetic etiology (hereditary pancreatitis). Hypertriglyceridemia can be associated to AP if serum triglyceride level reaches 1000 mg/ dl. Current opinion believes that the occurrence of AP is caused by the underlying derangement of lipid metabolism rather than by pancreatitis causing hyperlipidemia.
1.2 Basic pathophysiology of AP
AP consists in the autodigestion of the pancreas by prematurely, inappropriately trypsinogen activation. The pathophysiology of AP develops in three steps. The first step is characterized by trigger of inflammation, caused by various agents: biliary, alcoholic, hypercalcemia, hypertriglyceridemia, obstructive, pancreatitis gene mutations. Therefore some intracellular injuries follow such as cellular membrane trafficking alteration, zymogen and lysosomal granule fuse activate trypsinogen to trypsin and finally intracellular trypsin triggers the zymogen activation cascade [10,11]. The second step encompasses the systemic inflammatory response. Secretory vesicles, extruded into interstitium act as chemoattractants for inflammatory cells as neutrophils macrophages. Trypsinogen and activated digestive enzymes can be drained in the blood circulation. The digestive enzymes activation can be limited, followed by edematous pancreatitis or, on the contrary, massive with necrotic pancreatitis. Activated neutrophils release proteolytic enzymes (cathepsins); macrophages release cytokines (interleukin 6-8, TNF alpha). There are two possible evolutions of the phlogosis: local inflammatory response characterized by increased pancreatic vascular permeability and hemorrhage, edema, necrosis. On the other hand can develop systemic inflammatory response with systemic inflammatory response syndrome (SIRS), multiple organ dysfunction syndrome (MODS) and toxic phase [12]. The third step is characterized by systemic infection response. There are in evidence bacteremia by intestinal flora translocation with secondary infection of fluidnecrotic (peri) pancreatic collections that make up the septic phase. The predominant pathological event in this phase is the development of compensatory anti-inflammatory response syndrome (CARS) that is a systemic deactivation of the immune system.
In the presentation of the diagnostic and therapeutic sections of this complex disease can be useful to clarify some definitions. We can discover the corriespondence between pathological evolution, imaging appearance and clinical presentation. For pathological features of parenchymal edema the imaging definition is acute edematous pancreatitis and clinical definition is mild pancreatitis. For pathological features of parenchymal necrosis, peripancreatic fat necrosis and hemorrhage, peripancreatic fluid-necrotic collections the imaging definition is hemorrhagic necrotic pancreatitis and clinical definition is moderate/severe pancreatitis with single organ failure, minor systemic impairment; or can be also severe/early severe pancreatitis with multiple organ failure, SIRS, septic shock.
In the AP the clinical forms of different severity show various possible developments. Clinical evolutions of AP encompass for mild pancreatitis most frequently self-restoring. It’s possible, if, in biliary etiology, there is persistent impaired flow through duodenal papilla, to occur recurrent pancreatitis. Recurrent pancreatitis can occur also in the evolution of moderate/severe forms. Moderate/severe and severe pancreatitis can develop a favorable evolution as self-restoring of fluid collections. The less favorable evolutions encompass septic invasion of fluid – necrotic collections, pancreatic abscess, walled of necrosis. Finally the late unusual evolution of not complicated fluid gatherings is the acute postnecrotic pseudocyst.
2. Patients and Methods
The mild pancreatitis is the most frequent clinical presentation of the disease. A detailed history and a careful clinical examination may reveal the characteristic signs and symptoms of the disease. In the history should be reported previous biliary colic, alcohol abuse, dyspeptic discomfort, family history of hypertriglyceridemia. The abdominal clinical signs and symptoms can be set as a specific impairment: pains centrally located, such as in the biliary colic or localized on either side of the abdomen, typically radiated to the back; abdominal distension, decrease or absent bowel sound, abdominal tenderness or muscular guarding. There are also signs of the moderate involvement of the general conditions: fever, tachycardia, tachypnea, dispnea, mild hypotension. More specific for biliary etiology should be the jaundice. The diagnostic criteria include specific laboratory data such as increased values of pancreatic amylase and lipase. Serum amylase increases at the onset of the disease and decreases in a few days (3-5 days); on the contrary the lipase tends to remain elevated for longer. The increased level of serum amylase has not correlation with severity of pancreatitis. Liver function tests, cholestasis indexes, fasting serum calcium and lipid profile contribute to define the biliary etiology of pancreatitis. In the evaluation of AP and its clinical course, imaging exams play a central role. Abdominal ultrasound (US) may demonstrate gallbladder lithiasis and/or gallstones, sludge, microlithiasis in the common bile duct (CBD) with its dilation (more than 8 mm) or a real impacted stone in the CBD, involvement in the pancreatic site. The contrast enhanced computed tomography (CECT) and magnetic resonance imaging (MRI) are considered second level exams, with the aim to evaluate the damage of the pancreatic parenchyma, the involvement of the pancreatic tissue, presence of fluid-necrotic collections. Moreover CECT and MRI can confirm the detection of bile stones or CBD dilation that give us the possible diagnosis of biliary origin of pancreatitis. The CECT is currently employed for the assessment of pancreatic damage following the grade scale of computed tomography severity index (CTSI) of Balthazar [13]. There is within the second level exams also the endoscopic ultrasonography (EUS). This instrumental test can be very useful in the assessment of AP for the detection of CBD microlithiasis and periampullary lesions [14].
The assessment of homogeneous clinical cases should better define the diagnostic and therapeutic program. In the Service of General Surgery of University of Foggia (Italy) we observed and treated 351 cases of acute pancreatitis. Very less frequent are the acute presentation of chronic pancreatitis (Table 2). The clinical appearance of AP is a mild-moderate disease in the majority of patients (80%). The severe form occurs in 20% of patients. The first assessment based on clinical appearance and basic laboratory exams allows the diagnosis of acute episode of pancreatitis. The first level etiological assessment by percentage incidence of biliary lithiasis and cholestasis indexes showed biliary etiology in 339 patients (Table 3). In our experience is most frequent the biliary etiology and the majority of our patients present the mild-moderate forms. We have assessed our patients based on CT severity index, CT grade point + point for necrosis (Table 4). Our observations have shown 76% of the patients with mild or moderate/severe forms (grade B1,C2) and 24% with severe and early severe forms (grade D3,E4). Regarding the point for necrosis 19 patients have shown 30%-50% of necrosis in parenchymal tissue; 71 patients with less than 30% of necrosis, whereas 249 patients don’t have pancreatic necrosis. Moreover the comparison of the clinical appearance between early severe AP(ESAP) and severe AP(SAP) can define the clinical forms of disease of different severity and allows to define the better therapeutic approach (Table 5). The degree of pancreas involvement based on Balthazar score was more high in the clinical forms of pancreatitis that can be defined early severe. These forms are characterized also by major incidence of MODS, pancreatic sepsis, hypoxaemia and mortality. In summary, by clinical evaluation, we can identify within AP, early severe forms with major global impairment and severe forms with lesser general damage.



In the diagnostic phase of AP the first essential step is the early assessment of severity. The central question is: there are some predictive tests of severity evolution? These tests can be divided into direct and indirect. The direct factors are morphologic, based on anatomical compromission of the pancreas, assessed by imaging exams (US,CT,MRI). Unfortunately these are valuable not at the start of the disease, but after the complete evolution of the pancreatic involvement, usually 24-48 hours after the onset. The indirect methods may be mono or multifactorial (single or multiple laboratory markers). In table 6 [15] we report the monofactorial markers, more reported in the literature. Among these are reliable and very early CRP, urinary trypsinogen activation peptide (TAP), procalcitonin, Hct, all with high sensibility and specificity. The multifactorial prognostic scoring systems encompass Ranson, Glasgow (specific for AP) and APACHE II scores. The single factors are reliable at the onset of the pancreatitis attack; on the contrary multifactorial scores are active and effective late, after 24-48 hours from the onset, when the general impairment has already been achieved. The morphological evaluations of (peri) pancreatic damage by imaging exams are critical for the prognostic-therapeutic definition, but are not useful for early assessment of severity because the complete evolution of (peri) pancreatic involvement usually develops 24-48 hours after the onset. The correct definition of (peri) pancreatic damage with CT images can be reached by use of CTSI + point for necrosis and modified CT severity index (MCTSI) [13,16-18].

SAP usually appears as a biphasic disease. The first phase (firstsecond week) is characterized by evident abdominal pain, distension, tenderness or muscular guarding, hemodynamic instability, tachypnea, hypotension, dispnea, hemoconcentration. Typical of the severe forms is the early impairment of general conditions, hypoxaemia, beginning of toxic- enzymatic phase with single/multiple organ failure, SIRS, MODS. There are by laboratory tests confirmation of severe general impairment and by imaging exams evidence of severe (peri) pancreatic damage. In the later phase develop and evolue (peri) pancreatic fluid-necrotic gatherings and their septic complications.
Biliary is most common cause of AP. In our experience acute biliary pancreatitis (ABP) is in great evidence. The etiological assessment can be a guide in the therapeutic programs. Early etiological definition of AP can be proposed for biliary and alcoholic forms. The clinical appearance of ABP should be defined by previous history of biliary colic, jaundice and symptoms and signs of cholangitis. Laboratory study can show increased level of serum amylase and lipase three time upper normal, fasting serum calcium, lipid profile, pathological changes in liver function tests: increase of alanine transaminase has positive predictive value of 95% in the diagnosis of ABP. Crucial is the detection of the increased bilirubin and cholestasis tests. Imaging exams (US, CT, MRI) play a central role in the etiological assessment of pancreatitis: gallbladder lithiasis, stones, sludge, microlithiasis in CBD, CBD dilation more than 8 mm, impacted CBD stones. The imaging exams play also the diagnostic role in the assessment of pancreatic damage: parenchymal edema, necrosis, fluid-necrotic gatherings, etc.
There are also in our experience the acute presentation of chronic pancreatitis that can be a clinical pitfall in the comparison of true AP. Chronic pancreatitis can be usually connected with alcohol abuse. The typical clinical features of acute presentation of chronic pancreatitis encompass history of abitual alcohol abuse (over 5-15 years), acute relapsing attack, with severe abdominal pains, nausea, vomiting, tachycardia, tachypnea, usually without severe involvement of general conditions. Laboratory data relating to phlogistic disease, are not diagnostic for etiology; increased level of serum amylase and lipase. Imaging exams (US, CT, MRI, EUS) can detect usually lesions of chronic pancreatitis: parenchymal calcifications, dilation of main pancreatic duct (more or equal 3,5 mm), irregular contour of pancreatic duct, dilated side-branches (more or equal 1 mm). Alcohol etiology don’t cause, or is a very rare event, acute severe autonomous pancreatitis with (peri) pancreatic damage (necrosis, fluid-necrotic collections), but usually can develop an acute exacerbation of chronic pancreatitis.
3. Results
The first approach in mild forms of AP, from any etiology, usually requires intravenous fluid replacement, control of abdominal pains, sometimes by narcotic analgesic, gastric antisecretory medications, with holding oral diet. The use of nasogastric decompression and prophylactic antibiotics is debatable. The mild forms of AP have been defined as self-restoring forms, because these basic, simple therapeutic measures.
More complex, on the contrary, is the first approach in the moderate/ severe and severe forms of AP. In the clinical forms with impairment of general conditions, with an early toxic-enzymatic injury and SIRS with possible single or multiple organ failure, can be required resuscitative measures that encompass aggressive intravenous hydratation, guided by evidence of end organ perfusion (e.g. urine output) and control of cardiovascular and renal comorbidities; for these patients can be possible the admission in intensive care unit (ICU). Very important in these phases is the nutritional support. Enteral nutrition should be preferred to avoid intestinal impairment and to prevent complications infections. However should be limited the parenteral nutrition followed by suspension of intestinal activity. The employ of prophylactic antibiotic is actually under discussion, although their use is widespread. The revision of Atlanta criteria indicated that the pancreatic necrosis can be a risk factor for worsening of SAP and some data from the literature suggest that it may occur also with minimal pancreatic necrosis. The late phase (third-fourth week) follows and can occur septic complications of necrotic tissue and the appearance of (peri) pancreatic fluid-necrotic collections.
From our experience is in evidence the treatment of ABP that is well defined. The therapeutic cornerstone in the ABP is the control and correction of impaired biliopancreatic flow by ERCP and ES. This therapeutic procedure must be preceded by confirmation of papillary or CBD obstacle (stones, sludge, microlithiasis, papillary sclerosis) or cholestasis, CBD dilation, cholangitis, based on laboratory tests and imaging exams. The clinical presentation of ABP is very variable and we need to define the indications of ERCP/ES. We can define in detail the direction and use of ERCP/ES: (1) which patients should be submitted to procedure (2) the timing of procedure (3) the complications of procedure (4) the results of procedure. Based on our experience the patients that should be submitted to ERCP/ ES are the following: (1) all patients with severe, early severe acute biliary pancreatitis (2) all patients with recurrent pancreatitis (3) several patients with moderate or moderate/severe pancreatitis. It’s mandatory, prior of the procedure, to confirm the cholestasis, CBD or papillary obstacle by laboratory and imaging exams. Can be useful, to clarify this complex and debated therapeutic problem, to show our personal experience in the use and indications of ERCP/ES in acute biliary pancreatitis. We follow the phases of the development of the severe, moderate/severe pancreatitis in performing the therapeutic program. In the first phase the main procedure is the ERCP/ES, within 72 hours from the onset, with the details shown in the table 7. In all patients with ABP, submitted or not to ES, it is indicated to perform in the same hospital stay the laparoscopic cholecystectomy (LC) to complete the therapeutic program. The time of cholecystectomy is connected with AP evolution, because it is preferable to wait for the stabilization and improvement of the general conditions and of phlogistic impairment of (peri) pancreatic tissue [19]. In the second phase of the therapeutic program of SAP-ESAP there is the control and treatment of (peri) pancreatic fluid-necrotic gatherings (Table 8). More than 80% of these patients showed the spontaneous resolution of fluid-necrotic collections. On the contrary only 16,4% of patients needs to interventional procedures.


For the patients, submitted or not to ERCP/ES, we have performed a follow-up program with clinical, laboratory and imaging control at 3 and 6 months after hospital discarge. The aim of the follow-up was to assess the possible functional alterations following the ES. Among the patients with the severe or moderate/severe ABP, underwent to sphincterotomy, the follow-up program has been performed in 58,94% of the patients: these delayed controls did not show abnormal data (Table 9). Similarly we found also normal data at delayed controls, among the patients with mild-moderate ABP, not submitted to ERCP/ ES (Table 10). These results should confirm our right choice of the patients submitted or not to procedure.


4. Discussion
Now we can make a summary of this complex therapeutic problem, overall about the reasons of the therapeutic choice. The diagnostic sequence is clear: biliary etiology of pancreatitis can be early established by history, laboratory and imaging studies; confirmation of papillary obstacle, persistent or transient, and cholangitis concomitant to pancreatitis. For the following therapeutic choice of ERCP/ES there is evidence from the literature by historical contributions [20-23] and more recent systematic reviews [24-30]. The conclusions of these studies agree on some points: (1) early ERCP/ES has not advantage for patients with mild pancreatitis and is not indicated (2) early ERCP/ ES may be indicated in patients with severe disease, with or without biliary obstruction or cholangitis and in the disease with clinical evidence of cholestasis or cholangitis. Moreover several studies [26-29] suggest wider therapeutic indications with better results: early ERCP/ES reduce local and systemic complications and mortality, even if without statistical significance, in patients with predicted severe pancreatitis. There remain two arguments to consider: the timing and complications of ERCP/ES. The timing of ERCP/ES should be chosen within the first 48-72 hours from the onset of the pancreatic attack. Some data from the literature [31] suggest that the severity of pancreatitis is related to the duration of biliopancreatic ductal obstruction. Consequently there is the indication to perform the ERCP/ES early after the onset of symptoms [32]. A randomized controlled trial, now in course, [33] should perform the evaluation of the comparison of early biliary decompression versus conservative treatment in ABP. Finally there is the particular condition: ERCP/ ES in the patients with SAP, severe impairment of general conditions and requirement of intensive care and assisted ventilation can be high risk procedure. This therapeutic choice is very difficult and without worldwide consent. The complications of ERCP/ES are not unusual and include post-procedural pancreatitis, perforations, bleeding, and infections. The incidence rate of all complications is 10%; the incidence rate of major morbidity is 1,5%; the mortality reaches less than 0,5%.
The therapeutic choices in later phase of SAP are based on the development and evolution of (peri) pancreatic fluid-necrotic gatherings and their septic complications [34]. The pathological basis of therapeutic program in the SAP are linked on the grade of impairment of pancreatic parenchyma and peripancreatic tissue. The advanced phase of SAP is characterized by a counteractive antiinflammatory response syndrome (CARS) with the risk of infected necrosis and worsening of organ failure. SAP in its late phase can have some, diversified evolutions: (1) amelioration of early organ failure after intensive care but infection of (peri) pancreatic necrotic tissues causes worsening of general conditions in the second, late phase of the disease (2) uninterrupted serious conditions without improvement between the first phase of early organ failure and the infected necrosis in the following third- fourth week (4) persistent organ failure that also requires control of necrotic fluid collections infection by fine needle aspiration bacteriology (FNAB), and gas bubbles on CECT: if confirmation of septic complication, interventional procedures should be employed. The necrotic collections of SAP show some pathological features. The necrotizing pancreatic tissues are characterized by hypoperfusion of the parenchyma, detected by CECT; the prevalence of necrotizing forms is 15%-20%. The necrotizing process involves the gland parenchyma and peripancreatic tissues with very variable extension. The extensive interstitial edema is associated with (peri) pancreatic necrosis in a short period of 48-72 hours after the onset of the acute attack. These inflammatory, necrotic tissues give rise to acute, postnecrotic fluid collections with an amount of devitalized tissues. The further evolution of these fluid gatherings is characterized by demarcation between viable and necrotic tissues and the limit is set with a wall of granulation tissue.
The therapeutic perspectives are the most debated problem and include several specific decisions based on some questions. Should be identified some key points that can clarify the whole therapeutic program. Not complicated and asymptomatic fluid-necrotic gatherings should be submitted to observation and conservative procedures. In these clinical conditions the surgical manoeuvres should be avoided. In the follow-up program can be important to single out the early signs of infection in the fluid-necrotic collections. There are the well known clinical and laboratory signs of sepsis. On CECT can be detected suspicious images of infection such as gas bubbles in the area of fluid collections. Only if there is a doubt can be performed the FNAB. In some patients with infection in the fluid-necrotic collections, submitted to general antimicrobial therapy, can be absent amelioration of general conditions. In these patients can be useful to delay the surgical approach, also for some weeks, to wait the favorable evolution of demarcation of the collection, so-called walled-off necrosis. This established procedure is very important. There is almost unanimous consensus to delay the intervention until the fluid-necrotic collections are encapsulated, that is walled-off necrosis [35-37]. Early surgery, first week from the onset of the disease shows debatable results with high mortality rate (to 75%); the later procedures are, on the contrary, characterized by considerable decrease of mortality to 5% [38]. Finally the last point regards the choice of the surgical approach for the treatment of fluid-necrotic complicated collections. The surgery showed a progressive evolution to mininvasive, followed by better results and minor mortality than the open necrosectomy [39]. There are many mininvasive surgical procedures for the treatment of walled-off pancreatic necrosis: percutaneous drainage, endoscopic drainage, endoscopic necrosectomy, necrosectomy with minimally invasive step-up approach, endoscopic transluminal necrosectomy (ETN), video assisted retroperitoneal debridement (VARD), transgastric debridement, laparoscopic transabdominal debridement, opendebridement.The better identification of the collections, for the endoscopic approaches, can be obtained with the use of EUS [40].
Finally unusual evolution of fluid-necrotic collections, without septic complications, in SAP is the acute postnecrotic pseudocysts. The acute postnecrotic pseudocysts have incidence that ranges from 5% to 16% [41]. The evolution of these lesions can be very long to form (12-16 weeks). The treatment is required if the lesion is larger than 6-7 cm, symptomatic and persistent over many months. Within the mini invasive approach the EUS plays nowadays a central role in the management of acute pancreatic pseudocysts. The conventional transmural drainage has been improved today as EUS-guided transmural drainage. The advantages of EUS-guided procedure are evident: precise detection of distance between gastric lumen and pseudocysts and possible presence in this site of vascular structures; it’s also possible to localize the non-bulging pseudocysts and to show the lack of solid or necrotic components in the pseudocysts [40,42]. The rational basis of treatment is the accomplishment of cystic digestive prolonged connection.
5. Conclusion
In the severe, moderate/severe, recurrent acute pancreatitis with clinical, laboratory, instrumental confirmation of cholestasis, cholangitis, papillary or CBD obstacle is indicated the therapeutic ERCP/ES within 72 hours. In septic necrotic collections the role of the surgery should be limited, as first approach, to percutaneous drainage (that in most cases could reduce the need for surgery). If major surgical interventions are required, these should be more conservative as possible and preferred minimally invasive approaches.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
N Tartaglia, A Fersini , P Cianci ,A Ambrosi are involved in revising
the manuscript critically on important intellectual contents.
V Neri make substantial contributions to the conception and design
of study and evaluation, analysis of data; he wrote the paper.