


1. Background
Celiac disease (CD) is an autoimmune enteropathy that affects genetically susceptible individuals, following exposure to gluten, a component of wheat, barley and rye. CD is characterized by typical lesions of the duodenal mucosa. The histological features include villous atrophy, crypt hyperplasia, mononuclear cell infiltration of the lamina propria and an increase in the number of intraepithelial lymphocytes (IEL).
Recent studies revealed that CD affects > 1% of the general population, both in Europe [1,2] and in North America [3], where its prevalence has increased sharply in recent decades, with up to 4-fold increase in the past fifty years [4].
It is often difficult to recognize CD due to the variability of its clinical features and symptoms. In fact, CD can appear with gastrointestinal symptoms (typical form), in patients with extra-intestinal symptoms, such as headaches, recurrent aphthous stomatitis, dermatitis herpetiformis, iron-deficiency anemia (atypical form) or be asymptomatic (silent form). The clinical picture of CD can also be dominated by the other autoimmune conditions that are associated with it [5,6].
Highly sensitive and specific serologic tests are available to screen for CD. Those currently recommended are anti-gliadin deamidated (AGAD), anti-endomysium (EMA) and anti- human transglutaminase antibodies (tTG Ab). The demonstration of histological changes of the small bowel mucosa, evaluated according to the Marsh classification as modified by Oberhuber et al, is the criterion standard for CD diagnosis [7].
In celiac patients an involvement of the other parts of the digestive tract was also described, such as gastric [8-11], duodenal bulb [12] and colonic mucosa [13].
Helicobacter pylori (Hp) is the causative agent in more than 90% of cases of chronic gastritis, peptic ulcer disease, primary gastric mucosa-associated lymphoid tissue (MALT) lymphoma and gastric cancer [14,15]. Hp has evolved numerous strategies to enable its survival and persistence within the gastric mucosa including Several studies have shown that the prevalence of Hp infection is decreasing in adults and children in many countries [16,17]. This is attributed to improvement in socioeconomic status (number of family members per household, siblings sharing a bed, bathing facilities) and possibly antibiotic use.
Although Hp is one of the most common bacteria that colonize humans, the majority of infected individuals remain asymptomatic. A complex combination of host, environmental and bacteria factors are considered to determine susceptibility and severity of outcome in the subset of individuals that develop clinical disease.
Invasive and non-invasive tests are available for the Hp diagnosis [18]. Invasive tests include histology (the gold standard in the direct diagnosis of Hp gastritis), rapid urease test (RUT) with an accuracy of >90% in the detection of Hp infection, PCR and real-time PCR for the detection o mutations leading to resistance and culture associated with antibiotic susceptibility testing that should be performed after the first eradication failure before providing second-line treatment [18]. Non-invasive tests include C13 urea breath test with a diagnostic accuracy of >95% but it is less accurate for the diagnosis in young children [19], monoclonal stool antigen test (SAT) and antibodybased test with a relatively high negative predictive value [18]. The selection of the most suitable diagnostic test depends on the clinical circumstances as well as on their availability and cost.
The purpose of this short review is to assess the possible relationship between Hp infection and celiac disease.
2. Materials and Method
Studies were identified by searching PubMed, SCOPUS and Directory of Open Access Journal (DOAJ) databases. The last search was run on May 2014.
We used the following search terms for all databases: “celiac disease and Helicobacter pylori”.
We included retrospective and prospective studies and cross-sectional study from 1996 to May 2014, written in English. Additional papers were selected by a manual search of the reference lists of the retrieved articles. We excluded review articles, meta-analyses, case reports and editorials.
3. Results and Discussion
The search for Medline, Scopus and DOAJ provided a total of 530 citation. After adjusting for duplicates 509 remained. Of these, 475 were discarded because the title and/or the abstract were off-topic. Nine full text were excluded because the articles are not written in English or because they were reviews, case reports, editorials or meta-analyses. Seventeen studies met the inclusion criteria and were included in quantitative analysis (Figure 1).

We included eleven articles from Europe, three from Asia and three from American continent.
Over the past few years, several studies was performed to evaluate the relationship between celiac disease and Hp infection but the results are still controversial.
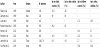
Hp infection is the most prevalent gastrointestinal infection worldwide. The prevalence of Hp infection differs widely in different geographic regions and over the years has shown a downward trend (Table 1).
The majority of cases are asymptomatic but histological evidence of chronic gastritis is present almost universally. Several authors also a correlation with lymphocytic gastritis (LG) which is also the most frequent form of gastritis observed in celiac patients [8-11,20,21].
A recent study by Guz-Mark et al. reported a prevalence of Hp infection by 30.6% in their series of 306 younger celiac patients. No significance difference in IEL counts according to Hp positive or negative was found, suggesting that Hp status is irrelevant for CD diagnosis. These findings are consistent with those reported by Villanacci et al. among adult celiac patients. However, 85% of patients in both group had IEL counts higher than 40 IELs/100. In patients without CD, Hp had a marginal effect on the duodenal IEL counts, from an average of 15 IELs/100 to 17 (Hp negative vs. Hp positive respectively). The authors also showed a slight trend among the positive Hp patients to have more severe villous atrophy [21]. This finding contrasts those of both Villanacci and Aydogu, who reported higher rates of low-grade lesions among positive Hp celiac patients [22,23].
In contrast to the Guz-Mark study, Memeo et al. reported an increase in IEL count in their group of 50 Hp positive adult patients compared with 30 Hp negative patients but this study used a lower limit of IELs (20 IEL/100) and only few patients were tested for CD [24].
Some studies described a correlation between Hp infection and the increase of gastric and duodenal IEL without villous atrophy [20,25]. Moreover both studies showed that Hp eradication is associated with a decrease in both gastric and duodenal IEL count, suggesting that duodenal intraepithelial lymphocytosis outside CD may be the result of an immune response to luminal antigens, such as Hp, analogous to the response to gluten in celiac patients.
Rostami-Nejad et al. performed a study on 450 adults who underwent upper endoscopy for dyspeptic symptoms. The prevalence of Hp infection among 28 CD patients and in patients without CD was 82% and 86.2% respectively. The difference is not statistically significant, according to previous studies by Diamanti et al. and Luzza et al. that showed a difference in terms of prevalence not statistically significant [27,28,29]. In addition there was no relation between gastritis and severity of mucosal damage in CD.
The study of Santarelli et al. confirms the data that there is not a significant association between Hp infection and CD among a group of 85 patients with Hp infection and concomitant evidence of untreated CD [30].
In our study in 2012 Hp infection was found in 2.6% of celiac children and in 16% of control group. We also found a lower prevalence of Hp in celiac patients with chronic superficial gastritis (CSG) (8.3%) compared to the control group with CSG (64%). According to these data, we hypothesized that the pathogenesis of gastric damage in CD may be due to other factors, possibly including the delay of gastric emptying, which is reported in 30% to 60% of celiac [31]. Furthermore the study showed an Hp prevalence in celiacs with LG of 6.2% similar to that found by Prasad et al. (6%) [9]. Hayat et al. also noted that Hp infection play a role in the pathogenesis of LG also in patients without CD and its eradication may lead to a significant reduction in the number of IEL, not confirmed by other studies [10]. In our another study of the same year no patients with Hp infection both in celiac and controls showed LG, suggesting that the role of the bacterium in LG is quite marginal. Moreover in our series higher prevalence of Hp infection has been reported in adults than in children and in controls than celiacs according to Lebwohl et al. [32,26].
4. Conclusion
The results variability of the different studies is probably due to large differences in Hp prevalence, small series of patients, lack of histological confirmation of Hp in some studies and lack of adjustment for sociodemographic characteristics. In addition, many geographic areas are not represented in the studies examined. It is therefore necessary to perform further multicenter trials to clarify the possible unambiguous correlation between these two conditions.
Competing Interests
Authors have no conflicts of interest or financial ties to disclose.
Author Contributions
Dr. Stefano Pontone works with conception, design and drafting of the article, Dr. Laura Petrarca, Manuela Brighi and Maya Tonda performed the data collection. Dr. Gerarda Mastrogiorgio made the analysis and drafting of the article and Dr. Raffaella Nenna made the revision the manuscript, final approval.