


1. Introduction
Cervical cancer (CC) is the third most frequent neoplasm among women worldwide. In recent years, the etiology of the CC has been largely defined, identifying the human papillomavirus (HPV) as the etiological agent necessary for its development [1,2]. HPV infection is the most frequent sexually transmitted infection. At least 50% of the sexually active population could acquire it at some point in their lives [1].
The HPV genotype is known as a critical factor for the progression of infection to the CC [3]. Of the 150 HPV genotypes currently known, the International Agency for Research on Cancer (IARC) concludes that there is enough scientific evidence to confirm the carcinogenicity in the cervix of 12 of them, specifically genotypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58 and 59. Only two of these oncogenic high risk genotypes, 16 and 18, cause approximately 70% of the cases of cancer associated with HPV in the world. Genotypes 6 and 11 are considered low risk and are related to 95% of cases of genital warts. Currently, new genotypes have been incorporated into the different risk groups. The five most prevalent types of HPV in the world are HPV 16, 18, 52, 31, 58. The rest of the types have a prevalence of 0.6% or lower, including the genotype 45, as well as types 6 and 11 , associated with genital warts. In Europe, HPV 16 accounts for 66% of CC cases, followed by HPV 18 and HPV 33, with 7% and 6% respectively.
However, infection by different genotypes of HPV has a different prevalence depending on the population studied, which could significantly influence the results of prevention of CC with current vaccines. The presence of endogenous factors, those related to the host (endogenous hormones, genetic and immunological factors) and those specific to the virus (type of HPV, coinfections with other types of HPV, viral load or viral integration) are probably related, although more studies are needed. On the other hand, it is also difficult to know the real prevalence of genital HPV infection because the cases diagnosed are not reported because most of the infections are asymptomatic and self-limited [1]. Nowadays, there are no national data of burden disease associated with HPV. The national estimations of the number of cases in different stages of HPV infection and its progression to CC have been obtained by standardizing to the Spanish population the age-specific rates of the different regional studies and regional cancer data. In general, 2,103 women with cervical cancer are diagnosed annually in our country, being the seventh most common cancer in women of any age in our country, and the second if we circumscribe the age range between 15 and 44 years. There are 739 deaths per year for this cause [2]. 55.8% of cases of cervical cancer in Spanish women are attributed to genotypes 16 and 18 of HPV [2]. The results of the Cleopatra study showed that the prevalence of HPV infection in a population of 3261 women in Spain is 14.3% (95% CI: 13.1-15.5). The prevalence of high-risk genotypes among the total sample was 12.2% (95% CI: 11.1-13.4), representing 84.0% of the HPVpositive samples. Certain differences in prevalence by age groups were noted, since the value was higher in women between 18 and 25 years old (28.8%, 95% CI: 26.6-31.1), than in women of different ages. More advanced (between 56 and 65 years, the prevalence was 7%).
The demonstration of the etiological role of HPV allows new strategies for primary and secondary prevention [4]. The prevention of CC is based on the detection and treatment of cervical lesions. Traditionally, cytology methods have been the basis of structured prevention programs. Population screening programs using cytology have demonstrated their effectiveness in reducing the incidence of CC, mortality and years of life lost [5,6] In addition, prior diagnosis and treatment of injuries in non-invasive phases can reduce the burden of disease and the costs of health care [7]. However, the negative aspects of screening, such as the psychological consequences of false positives, overtreatment and adverse reactions of vaccination, should be taken into account when creating programs promoting adherence to clinical practice guidelines [5].
Currently in Spain there is no common program for CC screening for the existence of different public health strategies in each of the 17 Autonomous Communities. Majority of CCU's screening programs are opportunistic, with non-optimal coverage and deficits in equity and efficiency. It is estimated that more than 60% of diagnosed cervical neoplasms relapse in women without previous screening or with inadequate screening. Establishing a population screening program for CC, both in Spain and in other European countries, should be a priority as it is exposed in the "European Guidelines for Quality Assurance in Cervical Cancer Screening".
Therefore, the latest advances in knowledge about screening tests, their effectiveness, guidelines and criteria for application and behavior in the face of abnormal results, justified the elaboration in 2014 of the "Cervical Cancer Prevention Guide". The progressive convergence of women vaccinated against HPV (primary prevention) that should continue to be screened for cervical cancer (secondary prevention) in the following years, requires incorporating more sensitive and effective tests. To this end, indicators should be used to evaluate the process and provide maximum benefit (cost-effectiveness), otherwise, the existence of suboptimal coverage both in primary and secondary prevention and the use of unsuitable screening tests can lead to an increase in cost without a reduction in incidence and mortality due to CC in Spain. These changes in the strategies of primary and secondary prevention create new scenarios, which force us to raise different patterns of clinical attitude in women with abnormal screening tests (for example, in women with positive HPV and negative cytology).
For all of the above, the objective of this preliminary study was to estimate the prevalence of HPV infection in women between 35 and 65 years of age with inadequate screening for CC. The vast majority of the Spanish Autonomous Communities have not fully implemented population screening so the preliminary results of the Rioja program in women with inadequate screening acquire great relevance for future prevention programs and for the impact that new HPV vaccines can offer. Compared with the Cleopatra study, the aim is to characterize and describe a population at higher risk of HPV infection, such as women with inadequate screening.
2. Methods
The present work is a descriptive study on 1000 asymptomatic women, between 35 and 65 years, without previous cytology for 3 years or more (inappropriate screening of CC) attended in the Riojan Health Service (SERIS).
El sistema de cribado de cáncer de cérvix en La Rioja aprovechó la base de datos del Programa de Cribado de Cáncer de Mama y se amplió incluyendo las mujeres de25 a 65 años.
The CC screening system in La Rioja took the database of the Breast Cancer Screening Program and it was expanded to include women from 25 to 65 years old. With this information they were listed by TSI (Individual Health Card) of the Riojan women included in that age group. An informative pamphlet was written and distributed to all Health Centers and Hospitals of La Rioja, sending letters to patients on November 17, 2005. In February 2011, the entire population of women had already been contacted between 25 and 65 years old.
For the elaboration of this work, between November 2014 and November 2015, those patients who were attended in the "Healthy Woman" program (CCC consultations), as well as those derived from Primary Care, were included as long as they met the entry conditions of the study.
Endocervical and exocervical samples were taken by swab according to standard techniques and were sent to the pathology laboratory for cytological study and to the external laboratory of GENÓMICA SAU microbiology for the study of the HPV and genotyping. All the samples were processed in the Pathological Anatomy Laboratory of San Pedro Hospital with Papanicolaou stain, using the terminology of the third edition of Bethesda 2014.Immunohistochemical determination of p16INK4a was used in women with borderline lesions between high and low grade. It’s detected when the pRb (retinoblastoma gene protein) is mutated, deleted or inactivated.
The study of HPV in the endo and exocervical samples was carried out at Genómica Laboratory SAU located in Madrid using the CLART® HPV2 technique from GENÓMICA SAU. It is a biology molecular technology based on microarrays, which detects and identifies 35 genotypes of HPV, including all high and low risk included in prophylactic vaccines. All the reagents as well as the equipment to perform the genotyping technique will be provided by GENÓMICA SAU to the Hospital during the study period. Once taken and identified, the samples were refrigerated until they were collected by laboratory personnel.
The exclusion criteria of the program were permanent or temporary. A permanent exclusion criterion was women's total hysterectomy and as temporary criteria, women without sexual relations or women who consult for gynecological symptoms.
In the present study, data on the sexual behavior of the participants were not collected because it is not the main objective of the study, leaving open the possibility of carrying out a study in the future. The risk factors most commonly associated with the acquisition of HPV according to scientific evidence can be summarized as: early onset of the sexual intercourse, acquisition of a new sexual partner, short interval between sexual partners, number of sexual partners (the greater the number, the greater risk), male sexual partner at risk (history of sex with men, frequentation of prostitutes, not being circumcised), the systematic use of condoms, the presence of other sexually transmitted diseases and the viral genotype. The last three will be analyzed in the study.
Estimations of incidence and prevalence were carried out with a point value and it’s 95% confidence interval. The description of qualitative variables was made expressing the absolute number and it’s relative frequency and the quantitative variables were described with their mean and standard deviation. All the tests were bilateral and significant p values less than 0.05 were considered as significant. The calculations were carried out with the help of the SPSS program version 21.0.
3. Results
3.1 Characteristics of the population under study
During the period of development of this work, 1000 women were studied, of which 1000 samples were obtained. Of these, they were considered valid for the study 997 because it wasn’t obtained sufficient DNA from the cervical sample for HPV amplification in 3 patients.
Regarding the demographic characteristics of the population, we found that the average age of the total of women included in the study was 47.36 years. 86.9% of patients are from Central, Northern or Southern Europe, 3.2% from South America, 6.5% from Eastern Europe, 2.5% from Africa, 0.1% of North America and 0.8% of Asia. 17.7% are nulliparous, while 82.3% of them have had one or more children. Among those who have had a child, the average parity is 1.89 children. 33.5% of the patients were menopausal and the average age of the menarche was 11.7 years. 29.9% used condoms, 24.5% did not use any contraceptive method, 12.9% used oral hormonal contraceptives, 7.1% used double method, 4.1% IUD, 4% vasectomy, 3.6% tubal ligation, 4% the contraceptive patch and 1.1% the subcutaneous implant. 67.8% of them are smokers, 26.4% nonsmokers and 5.8% ex-smokers. 61.3% live in urban areas (96.9% in Logroño and 3.1% in Calahorra), while 38.7% come from rural areas, being these differences statistically significant (p <0.001).
3.2 Prevalence of infection by different HPV genotypes
Of the 997 samples studied, 130 (13%) tested positive for HPV DNA. Of these, 102 were for HPV-HR, 49 for HPV-LR and 11 for HPVIR. Table 1 summarizes the data found indicating the percentages of HPV infection with their corresponding 95% confidence intervals. Likewise, in the last column the percentages of HPV infection are indicated with respect to the total of the study samples. In this sense it could be said that if the sample of the study is representative of the population of La Rioja, the data can be extrapolated and say that the population prevalence of infections by HPV-HR is 79.2% and it’s 95% CI. 71.5-85.3. In the same way, the prevalence of HPV-IR would be 8.5% (95% CI 4.8-14.7) and that of HPV-LR would be 38.5% (95% CI 30.5.47).
Regarding the study by genotypes of HPV, the most frequent regardless of the type of lesion is HPV 16 followed by 33, 6, 45, 18, 35, 39, 52, 58, 11, 53, 68, 31, 66, 56, 83, 51, 84, 42, 61, 70, 72, 59, 44, 64, 89, 40, 62, 71, 81, 85, 82 (Figure 1a). Stratifying the sample by risk, 16, 33, 45 and 18 were the genotypes that were most frequently amplified. A total of 35 different genotypes were detected (14 from hR, 17 from LR and 4 from RI).

The 62.30% of the patients presented infection by multiple genotypes of HPV while the remaining 37.7% had infections by a single genotype (figure 1b). Of the patients with infection by multiple genotypes, 56% of the women had infection by two genotypes, 12% had infection by three, 10% by four, 2% by five and one patient had infection by 6 genotypes of HPV. Of the 81 patients with infection by multiple HPV genotypes, 95.06% of them are infections with predominance of the HPV-HR genotype (figure 1b).
It must be borne in mind that the same patient can be positive for different genotypes at the same time; therefore, the total number of patients is not the sum of the positive values for each category of genotypic risk. In this sense, when there is multiple infection, the value with the highest risk will be assigned, finding a total HPV-HR of 102 (79.2%), 25 HPV-LR (19.2%) and 3 HPV-IR (2.3%).
The prevalence of cytological anomalies in any of its grades was 4.2% in the samples studied. All of them were infected with HPV except 3 patients with ASCUS cytology. Thus, our data show 16.7% ASCUS (atypical squamous cells of uncertain significance), 56.8% LSIL (low-grade squamous intraepithelial lesion), 21.4% HSIL (highgrade squamous intraepithelial lesion); and 7.1% ICC (Invasive Cervical Cancer). The American College of Pathologists (CAP) and the American Society of Colposcopy and Cervical Pathology (ASCCP) have established a new histopathological terminology called LAST (Lower Anogenital Squamous Terminology), which homologate the cytological and histological nomenclature in a dual and parallel classification and involves to ano-genital lesions, represented by the terms: HSIL and LSIL. This dual approach attempts to reflect the biological behavior of the lesions and has been included in the latest O.M.S classification for female genital tract neoplasms published in 2014.
3.3 Prevalence of HPV according to age groups
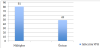
If we relate these results according to age, it is observed that in young women there is a higher prevalence of HPV compared to elderly women (17% vs. 11.4% vs. 6.1%) (figure 2).

4. Discussion
This is the first study of HPV prevalence in Spain in a population with inadequate screening and within the scope of the implementation of a structured population screening. The overall prevalence of 13% obtained in our community is in the high range of prevalences reported by other similar studies, as will be described below. In this regard, it should be noted that the majority of published Spanish studies come from opportunistic screening and carried out in the general population (selection of those patients with inadequate screening is not carried out, which would be precisely the high-risk patients) which may influence the results obtained. In this sense, the present study overestimates the prevalence of HPV because we focus on a population with inadequate screening, where both the prevalence of HPV and cytological lesions is usually higher, because it has not had a follow-up or received recommendations.
Both in a meta-analysis carried out with 78 works from around the world [8] and in the report issued by "HPV information center" in 2014 [9] it is estimated that the prevalence of HPV in Spanish women is 10.4% (95% CI 10.2-10.7), and 10.7% (95% CI 10-11.5), lower than those found in this study. This difference is probably due to the fact that patients with inadequate screening in La Rioja have a higher prevalence of HPV infection because of not having clinical follow-up.
Focusing on the studies carried out in our country, in an opportunistic study carried out in Galicia, in 1,703 women aged between 16 and 64 years coming from three gynecological centers and in a family planning center of the service of Galician health, found a prevalence of HPV of 10.1% (95% CI 8.6-11.6) [10]. Other studies carried out in Zaragoza [11], Madrid [12] or in the Basque Country [13] have been carried out in women with a previous pathological citoloy/biopsy or in women belonging to risk groups, such as sex workers [14], so that the results obtained in these studies could not be compared with those of the present work since the prevalences are much higher. In this sense, Bernal M et al. [11] concludes in its case-control study that there is a strong association between infection by genotypes 16 and 18 and CC, highlighting the importance of implanting vaccination against these genotypes to prevent CC. Martin P et al. [12] described a prevalence of 43.2% and concluded that HPV 16 was the most frequent in the region of Madrid, followed by HPV 53 and 31, with a lower prevalence of HPV 18. In this sense, although the vaccine against at HPV 16 and 18 can theoretically prevent 50% of HSIL cytological lesions, genotypes not included in the vaccine are frequent in their population. Therefore, it is necessary to know the distribution of genotypes to predict the effect of vaccines on the incidence of infection and evaluate cross protection.
In this sense, Bernal M et al. [11] concludes in its case-control study that there is a strong association between infection by genotypes 16 and 18 and CC, highlighting the importance of implanting vaccination against these genotypes to prevent CC. Martin P et al. [12] describes a prevalence of 43.2% and concludes that HPV 16 was more frequent in the Madrid region, followed by HPV 53 and 31, with a lower prevalence of HPV 18. Although the vaccine against HPV 16 and 18 can theoretically prevent 50% of HSIL cytological lesions, genotypes not included in the vaccine are common in their population. Therefore, it is necessary to know the distribution of genotypes to predict the effect of vaccines on the incidence of infection and to evaluate cross protection.
Finally, Delgado et al. [13] concludes that there is a high prevalence of infection by high-risk genotypes in patients with abnormalities in cytology with a global prevalence of 69.8%. In a study performed in Valladolid [15] it is observed that the prevalence of HPV correlates inversely with age. This goes from 42.7% in the group of women from 35 to 39 years to 8.9% in the group of 60-64 years. Our study confirms this relationship. Thus, the prevalence ranges from 16.98% in the group of women from 35 to 39 years to 6.06% in the group of 60-65 years. This decrease is linear from the group of 45-49 years with an approximate decrease of five percentage points of prevalence for each population range. This fact, together with the slow oncogenic progression of HPV, reinforces the fact that the beginning of molecular screening for HPV begins at 30-35 years of age. The difference between the age groups of the study (16% vs 11% vs 6%) is not as important as that found in the population with adequate CC screening of the Cleopatra Study. In this last work, differences in prevalence by age groups were observed, being higher in women between 18 and 25 years old (28.8%, 95% CI: 26.6-31.1), than in women of more advanced ages (9% in the group of 36 to 55 years and 7% in the group of 56 to 65 years). When analyzing if there are significant differences between age groups with regard to the Cleopatra study, that is, if the prevalence found in 36-45 years in the study (17%) is different from the prevalence in Cleopatra (9.5%) and so for each group, the differences are:
| Agegroups | Cleopatra | Elizalde, CR | p value |
| 36-45 | 9,5% | 17% | 0,006 |
| 46-55 | 8,6% | 11,4% | 0,004 |
| 56-65 | 7,0% | 6,1% | 0,64 |
In the younger age groups (36-45 and 46-55) the prevalence is higher in the present study than in that of Cleopatra (p <0.001), while there are no significant differences in the prevalence in the group. Aged 56 to 65 years (p = 0.64). In this study, a second peak was not observed in the 1950s or in the 1960s, as has been reported in other studies [16].
In comparison with the Cleopatra study, our work aims to characterize and describe a population at higher risk of HPV infection, such as women with inadequate screening, as discussed above. In this sense, both studies are not comparable although the prevalence for HPV infection are similar (14.3% Cleopatra). Among the virological data, it should be noted the low proportion of low risk HPV found. In spite of this, 38% of the women with HPV, had low-risk genotype, representing a third of the positive samples. In the remaining two thirds, 79.2% were high-risk HPV and 11% intermediate-risk. These proportions also include infections of more than one genotype, whether high, intermediate or low risk. 62.30% of the patients presented infection by multiple genotypes of HPV (81/130) while the remaining 37.7% had infections by a single genotype (49/130). The prevalence obtained in our work is double that obtained in the Cleopatra study (32.8%), which included a total of 3,155 women analyzed [17,18].
Other studies outside Spain report higher rates of multiple infections, up to 42.8%, although these studies focus on young women under 25 years of age [19] in whom the prevalence is higher. Therefore, these differences could be due to both the age and sexual behavior of the population studied as well as the geographical situation.
The scientific evidence shows that there are strong divergences in the most frequent type of virus in different areas. Most of the estimations are based on an initiative sponsored by the International Agency for Research on Cancer (IARC) in different parts of the world. There are differences by geographical area being higher in in Latin America - Colombia (15%), Chile (14%), Argentina (17%) and Costa Rica (16%) - and Africa - Nigeria (28%) - that in Asia - Vietnam (11% and 2%) and Thailand (6%), showing the European countries studied the lowest prevalences - Sweden (7%), and Spain (3%) - [2,5].
There is a wide variation in the HPV prevalences published in different countries, which reflects, in addition to the differences in HPV epidemiology, differences in the sampling strategies and the diagnostic techniques used. These data can be very useful, therefore, to develop vaccination programs, or specific diagnostic tests for each region. In a meta-analysis the data were analyzed by regions and it was observed that the presence of HPV is five times higher in sub- Saharan Africa than in Europe, while Asia and South America have intermediate rates [8].
The early age of onset of sexual intercourse with older men or with men who have multiple women, poor hygienic conditions and HIV infection may be some of the factors that explain this high prevalence of HPV. However, not only globally, but within each country and region, there are also differences in prevalence. Thus, we have found statistically significant differences between women who live in an urban environment and those who come from rural areas. However, there are no studies in the literature that describe results according to the rural or urban environment. Therefore, we can’t know the cause of these diferences.
Finally, it is important to mention that it is still not sufficiently clear whether infection with multiple types of HPV influences, either directly or immunologically, the persistence and progression of a type of HPV. In this regard and in relation to multiple HPV infections, the International Agency for Research on Cancer (IARC) performed HPV prevalence surveys in 15 areas on four different continents [20]. The data obtained came from 14,536 women recruited in the 15 areas, with an average age of 40.8 years, and obtained a lower percentage than that observed in La Rioja (32.2%) with respect to infection by multiple HPV genotypes. In this sense, some papers describe the possible influence of the test used in the screening [21] and, this, can explain, at least in part, the different results obtained. In addition, and as mentioned above, the fact that our study population is a high risk population due to inadequate screening can cause a higher percentage of multiple infections as well as high risk.
5. Conclusions
The overall prevalence of HPV positivity is 13% in women from La Rioja between 35 and 65 years with inadequate screening for CC. In addition, we found a higher prevalence of HPV-HR than low or intermediate risk. The majority of patients with positive HPV infection presented infection by multiple genotypes. However, it will be necessary to continue with the genotyping analysis to break down the lesions and the viral genotype involved in each lesion.
Our results are the first carried out within the scope of a structured population screening program in women with inadequate screening and should serve as a reference for future studies and to measure the future impact of vaccination. This preliminary study developed in our community is of great impact and interest to design future prevention programs and to analyze the effect that new vaccines can offer within the context of reducing the prevalence of cervical cancer.
Competing Interests
The authors declare that they have no competing interests.