


1. Introduction
Ectopic pregnancy is a public health issue all over the world, whatever the developmental status [1]. Its incidence varies between 1 to 2% of pregnancies [2]. Because of the recrudescence of sexually transmitted infections and smoking, this incidence has doubled even tripled from 1970 to 1990 in industrial countries [3]. In Europe these last years, the prognosis of ectopic pregnancy has subsequently improved due to diagnosis and therapeutic progress that have permitted reduction and even eradication of hemorrhaging accident from tubal rupture.
On the other hand, in developing countries, the frequency of ruptured ectopic pregnancy is still elevated and represents still the first cause of maternal mortality in the first trimester compromising further fertility [4,5,6]. This is related to late diagnosis, because in Africa women wait until three months amenorrhea to start antenatal care. In Benin in 2006, the frequency of ectopic pregnancy at the University clinic of gynecology and obstetric was 2.89% that is to say 1 case for 34 deliveries [7]. The impact of ectopic pregnancy on the maternal mortality during the first trimester is to be considered, since reaching 10% of the total maternal mortality [8]. According to PANEL L and DECHAUD H [3]. The ectopic pregnancy is life threatening: it represents 13% of maternal related death during the first trimester. For BOUTEVILLE C. and al [9], a woman having an ectopic pregnancy has a relative mortality risk 10 times higher than the one during delivery.
The aim of our study was to identify the risk factors and the prognosis of ruptured ectopic pregnancy at the University Clinic of gynecology and obstetrics at the National University Hospital Center Hubert K. Maga in Cotonou (Benin).
2. Patients and Procedure
It has been a retrospective and descriptive study ran over a 5 years period from the 1st January 2009 to the 31st December 2013. The study group was made up of childbearing age patients, consulting on their own or referred at the University Clinic of gynecology and obstetric. All patients received for ruptured ectopic pregnancy at the Emergency unit and treated at the University Clinic of gynecology and obstetric were included. The study has been conducted using the non-probability sampling method of commodity. Indeed, all patients’ files filling the selection criteria have been admitted in our study. The receptions records, of the Emergency care unit, orientation and of the operating room, files of patients selected, and the data processing form were made up of our means of data gathering. A pre-test was done on ten files, which helped us to correct the data processing form. We used these various records to list the patients’ files number filling the criteria. We then consulted the files at the University Clinic archives then analyzed to make an inventory of those that were complete. On a total of 336 files listed, 298 were included. The data collected on the data processing form were keyboarded and processed with the software EPIDATA. The confidentiality was respected and the anonymity of information’s relatives to each patient. The major difficulty was the absence of functional prognosis appreciation because many patients have been lost from sight.
3. Results
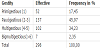
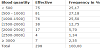
The frequency of ectopic pregnancy was 1.89% of the first trimester emergencies that is to say 1 case of ectopic pregnancy for 53 obstetrical emergencies. Among the 336 cases of ectopic pregnancies, the ruptured ectopic pregnancies accounted for 88.69% (298/336). During those 5 years, the progress of ruptured ectopic pregnancy was: 87.69% in 2009, 83.33% in 2010, 92.31% in 2011, 91.94% in 2012 and 88.46% in 2013. Our patients age varied between 16 and 45 years with an average of 28 years (28.48 standard deviation = 0.33). The dominant age bracket was between 20 and 29 (57.64%). 79.87% were unschooled. Married women accounted for 43.62% and single women for 6.7%. Craftswomen accounted for 42.62% followed by sellers 24.83%. 7.38% (n=22) had a history of cesarean section, 1.68% (n=5) had a history of appendectomy and 1, 34% (n=4) a history of myomectomy. On the 298 patients, 9.06% (n=27) had a history of ectopic pregnancy among which 22 had a history of salpingectomy and 6 of salpingotomy. The paucigravida dominated with 45.97% (table 1). The pauciparous represented the majority with 32.55% (n=97). The nulliparous and primiparous represent respectively 28.86% (n=86) and 24.50% (n=73). 30.54% (n=91) had no history of miscarriage and 8.39% (n=25) had history of induced abortion. Histories of genital infections (Tubal tuberculosis, gonococcia, chlamydiae, syphilis) were found in 42.95% (n=128). Among the 298 patients, 7.38% (n=22) were on contraceptive methods (4 IUD, and 18 under estroprogestative pills).The history of ovulation inductors were found in 0.67% (n=2). In our sample, 81.54% of patients were referred by peripheral centers. The patients’ dominant complaint was abdominal and pelvic pain with a percentage of 82.55%. Metrorrhagia was observed in 20.13% of patients. The most important number of ectopic pregnancy was ruptured between 7 and 10 weeks amenorrhea with a percentage of 39.60% (n=118). The extremes being between 3weeks and 19 weeks of amenorrhea. The dominant blood group and rhesus factors was O+ with 46.33% followed by A+ and B+ accounting respectively for 23.16% and 18.64%. The time limit of management was within the first two hours following admission for 36.58% and in a time limit of more than two hours in 42.28%. All patients had a laparotomy. The total salpingectomy was done in 88.25% (n=263) of the overall patients; Ovariectomy in 4.03% (n=12) and hysterectomy in 0.67% (n=2); conservative surgery in 7.05% (n=21). Haemoperitoneum was observed in all cases (Table 2). The tubal location was the most frequent (97.32%) with ampullar predominance in 56.71% of cases. Blood transfusion was done in 66.78% (n=199) of patients among which 56.71% had per operative autotransfusion by blood collection using Tanguieta funnel. The post operative was without complications in 86.24% (n=257) cases. Some post operative complications were registered especially decompensate anemia 9.73% (n=29) and endometritis 3.69% (n=11). After surgical management 10.74% (n=32) did not have proper quality tubes and were orientated to AMP, one case of maternal death, (0.34%) was registered. On 262 patients reviewed remotely from the operation, 94.32% (n=247) had had a pregnancy after the ectopic pregnancy. The time require for conception varied from 2months to 20 months after treatment of the ruptured ectopic pregnancy. Among these patients, 4 cases of relapse were noted.
4. Discussion
In our series, the dominant age bracket was from 20 to 29 years old (57.64%). This age bracket is similar to the one of PERRIN AND al [10] who found a dominant slice from 21 to 30 years old (61.27%). The ectopic pregnancy is therefore observed in young women and this is due to intense genital activity during that period and to desire for maternity. Pauciparous were the majority 32.55%. PERRIN R and al [10] from 1993 to 1994 in a study made at the University clinic of gynecology and obstetrics found that all women can be involve, but with a slight predominance of patients having had 1 or 2 pregnancies. This observation is also made by almost all the authors who estimate that ectopic pregnancy is associated to low parity [11,12]. We had collected 10.4% of cases with history of induced abortion. This rate is comparable with the one reported by RATINAHIRANA S. and al 8% [8] and more than the one of DIALLO F. B. and al [13] who found 3.28%. This difference can be explain by the behavioral change of young women in front of the notable amelioration of reproductive health with access to informations and advises. The history of genital infection in our study was 42.95%. PICAUD A. [14] had found 23%. Genital infections represent a major risk factor in ectopic pregnancy. They act on the uterine tubes peristaltic quality by making tissues inflammatory and the cilia less mobile. The most important number of ectopic pregnancy is ruptured between 7 and 10 weeks, 39.6% and the approximate results has been observed by MEYE J. F. and al [11], ODEJINMI F. and al [15] and MACRAE R and al [16]. This can be explained by the elevated frequency of ectopic pregnancy on the uterine tubes since the egg gets bigger and at this gestational age, the villosity development will cause tubal erosion and rupture. In our areas the pregnancy diagnosis is always late due to cultural beliefs of the society. Our patients prognosis has subsequently improved due to autotransfusion by peroperative blood collection using Taguieta funnel (56.71%). The resort to blood transfusion is frequent in cases of ruptured ectopic pregnancy. Therefore autotransfusion, a technique that consist of collecting intraperitoneal blood, compensate for the frequent blood shortage in Benin and to the numerous risk of homologous transfusion. The vital prognosis was good in immediate postoperative for 78.86%. Only one case of maternaldeathwasregistered. TIDIANE CISSE C. A. and al in Senegal [1], DIALLO F.B. and al [18], SELO OJEME O and al [19], had not registered cases of death in their series respectively. This lethality can be explained by the fact that our patient was admitted in hemorrhagic shock, she has not beneficiated of autotransfusion because of the infectious syndrome and blood shortage did not favor her. She died 6 hours after the surgery.
5. Conclusion
The ectopic pregnancy remains a public health issue. The risk factors mostly found are history of genital infection, adhesive bands secondary to pelvic surgery. Autotransfusion improves maternal prognosis.
6. Recommendation
To reduce the frequency of ruptured ectopic pregnancy and improve functional and vital prognosis in developing countries and in Benin particularly, we need early women consultation in cases of amenorrhea or suspected pregnancy to determine its location by a qualified health agent. Health agents most render good follow up of patients bearing genital infections.
Competing Interests
The authors declare that they have no competing interests.