


1. Introduction
Carcinosarcoma (malignant mixed muellerian tumor) of the ovary represents a rare and aggressive tumor entity. Carcinosarcomas of the ovary are about three times less prevalent than those of the uterus [1]. According to the WHO, carcinosarcomas are regarded as metaplastic carcinomas and are supposed to be of epithelial monoclonal origin.
The mesenchymal component of the carcinosarcoma either consists of homologous or heterologous elements. Homologous carcinosarcomas contain sarcomatous elements originating from tissue normally being present in the ovary. The heterologous components usually contain malignant osteoid, chondroid or rhabdomyoid cells. Overall, homologous sarcomatous tumors do not carry a better prognosis than the heterogenous counterparts [2-5].
The epithelial component more often represents multiple than singular components. Serous components are more common than endometrioid ones and have been demonstrated to be associated with an inferior prognosis in some studies [2]. Clear cell and squamous cancer components are rare. In the majority of cases, the development of metastases/tumor progression is caused by the epithelial component [6].
Staging of ovarian carcinosarcomas is carried out using that from ovarian cancers [7]. The prognosis of carcinosarcomas of the ovary is more favorable than that of the uterus [1]. However, they carry a significantly worse prognosis than (high-grade) serous carcinomas of the ovary [8-10].
Standard treatment of ovarian carcinosarcoma consists of bilateralsalpingo-oophorectomy, total abdominal hysterectomy, debulking of peritoneal metastases, and lymphadenectomy [1,2,9].
The present study retrospectively evaluated potential prognostic factors in a series of 26 consecutive patients with carcinosarcoma of the ovary diagnosed and treated at the Dept. of Obstetrics and Gynecology of the Medical University of Graz over a 25-year period.
2. Materials and Methods
26 consecutive patients with primary carcinosarcoma of the ovary were diagnosed and treated at the Department of Obstetrics and Gynecology of the Medical University of Graz, Austria, between 1987 and 2011. The following factors were retrospectively analyzed on the basis of an institutional computer data bank: Patient´s age, preoperative hemoglobin, platelet counts and lactate dehydrogenase, preoperative Karnofsky status, type of surgery, ascites, type of bowel involvement, FIGO stage, residual tumor, pelvic lymph node status, existence of a homologous or heterologous carcinosarcoma type, grade of differentiation, postoperative chemotherapy, localization of recurrence/metastasis, last date of follow-up and tumor status at last date of follow-up.
3. Results
Neither the univariate nor the multivariate analysis identified a subgroup of patients with favorable progression-free survival.
With regard to overall survival, univariate analysis revealed a favorable trend for patients < 70 years versus those > 70 years of age (5-year survival of 22% versus 0, respectively; p= 0.067). In addition, in patients with a preoperative lactate dehydrogenase (LDH)-value of < 200 U/L, a trend towards better overall survival was observed as compared to those with a LDH concentration of > 200 U/L (p= 0.052).
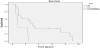
On multivariate analysis, age of the patients < 70 years was associated with an improved overall survival as compared to those > 70 years (34% versus 0 at 5 years, respectively; p= 0.008; Figure 1).
None of the other factors investigated including preoperative hemoglobin, platelet counts and lactate dehydrogenase, preoperative Karnofsky status, type of surgery, ascites, type of bowel involvement, FIGO stage, residual tumor, pelvic lymph node status, existence of a homologous or heterologous carcinosarcoma type, grade of differentiation, or postoperative chemotherapy revealed prognostic information.
All carcinosarcomas recurred or progressed. The sites of first recurrence are depicted in Table 1 the majority of them being located in the pelvis, parenchymal liver and peritoneum.

4. Discussion
Patients' age was the only factor being demonstrated to independently influence overall survival in the 26 patients with primary ovarian carcinosarcoma of stages I to III treated in the present study. Patients aged >70 years carried a significantly worse prognosis than younger patients (p= 0.008, Figure 1). This finding is supported by several other studies in which older patients also were found to exert a significantly worse survival rate [1,2,5,11].
Overall, prognosis of primary ovarian carcinosarcoma is particularly poor. Median survival was reported to range between seven and 26months, respectively. In the majority of studies, the median survival was around 11 months [1-5,9,14,15].
Similarly to the present study, also previous reports usually contained small numbers of patients only [2,3,5,12,16-19].
Higher disease stage was reported to negatively influence survival in the majority of studies reported [1,4,12,13,16,20-23].
Higher residual tumor burden has also been reported to be associated with an inferior prognosis [2,9,13-15,22,24]. In the present study, 69% of patients had optimal debulking surgery. Nevertheless, none of them survived five years without evidence of disease. This fact underlines the need of effective systemic therapy in carcinosarcomas of the ovary.
The use of platinum-based chemotherapy was found predictive of survival in some studies [11,13,15,21]. The combinations of cisplatinum and ifosfamide as well as carboplatin/paclitaxel have been studied more in detail [5,11,13-15,18,23]. However, there exists no adjuvant standard treatment for this disease.
This is the first (small) study which describes the patterns of initial recurrence/progression. There was a propensity towards pelvic, parenchymal liver, and peritoneal metastases in our cohort (Table 2). In contrast to classical epithelial ovarian cancer, the rate of parenchymal liver metastases as first site of recurrence seems was elevated (35%, Table 2).

5. Conclusion
In conclusion, the present study on carcinosarcoma of the ovary demonstrated age >70 years at diagnosis to be associated with a particularly unfavorable prognosis. Although carcinosarcomas are regarded to be of epithelial origin nowadays and thus are included in trials with epithelial ovarian cancer, the authors believe that this group should be analyzed separately due to its inferior prognosis and the urgent need for intensified research in this specific tumor entity.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Edgar Petru: Substantially contributed to the study conception and design.
Edgar Petru and Sanja Beganovic: contributed to the acquisition, analysis, and interpretation of data.
Vassiliki Kolovetsiou and Nora Woltsche: Drafting manuscript and approved the final version of the manuscript towards publication.