


1. Introduction
Psychological distress is defined as a state of emotional suffering associated with stressors and demands that are difficult to cope with in daily life . It is known to be associated with adverse health outcomes in various disease states and among different populations . Previous work indicates that psychological distress is associated with a 53% increased risk of hypertension after controlling for multiple risk factors of high blood pressure among the psychologically distressed adult USA population . Cardiovascular disease (CVD), including coronary heart disease (CHD) and stroke, is the leading cause of death for men, women, and people of most racial and ethnic groups in the United States [4]. The association between psychological distress and cardiovascular disease has not been extensively studied. The aim of this study is to examine the association of psychological distress and cardiovascular disease among the adult USA population based on data from the National Health Interview Survey (NHIS). NHIS is a principal source of information on the health of the civilian noninstitutionalized population of the United States [5]. We used data from 2004-2013 that included an assessment of psychological distress using the standardized Kessler-6 questionnaire [6].
2. Materials & Methods
Data was analyzed from the National Health Interview Survey (NHIS) administered by the CDC’s National Center for Health Statistics (NCHS) from 2004-2013. NHIS includes non-institutionalized American civilians sampled by household following a multi-stage area probability design. The survey included Kessler 6, a standardized psychological distress scale that is an abbreviated version of Kessler 10, which was used for screening and assessment of severity of anxiety disorders.
SPSS® version 26 was used for assessing measures of central tendency, and for analysis utilizing t-test and ANOVA for continuous variables. Data is presented as the mean ±SEM unless otherwise specified.
Chi-squared analysis was used for categorical variables. A logistic regression model was used to estimate the odds ratio and the strength of association between psychological distress and cardiovascular risk factors, myocardial infarction, and stroke. Both the unadjusted and adjusted odds ratio were calculated. The adjusted odds ratios adjusted for CVD risk factors including: age, Body mass index, Diabetes, Hypertension, Hypercholesterolemia, Smoking, Chronic Kidney Disease.
3. Results
Of the 284,497 respondents to the Kessler Psychological Distress Scale (K6) involved in our study representing the adult USA population, 10,218 (3.6%) reported psychological distress with a mean age of (years ±SEM) (48.09 ± 0.16 vs. 47.69 ± 0.04, p<0.05), for psychological distress vs. non-psychologically distressed groups respectively. Psychological distress tended to be more common among age group 45-64 years (4.4%) compared to those 18-44 (2.8%) and those more than 65 years of age (2.6%), p<0.01 (Table 1). Psychological distress was more prevalent among women compared to men (4.2% vs. 2.9% for women and men respectively, p=0.01). Hispanics and Blacks had higher percentage of psychological distress (4.1% vs. 4.0% vs. 3.5% vs. 1.9%, p<0.01) for Hispanics, Blacks, Whites, and Asians respectively. Psychological distress was more prevalent among those without high school degree (7.0% vs. 3.0%, p<0.01). The rate of psychological distress as it relates to alcohol drinking was (5.9% vs. 3.1% vs. 3.4%, p<0.01) for former drinkers, never drinkers and current drinkers respectively. Psychological distress was 3.4 times as prevalent among those who are below the federal poverty level (FPL), compared to those above the FPL (2.6% Vs 8.9%, P<0.01) for those above and below the FPL respectively.

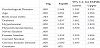
For risk factors of Cardiovascular disease (CVD) (Table 2), current smokers have greater psychological distress than former smokers and never smokers (7.5% vs. 3.2% vs. 2.4%, p<0.01 for current, former and never smokers respectively. There was no significant difference in the prevalence of psychological distress by exercise category (2.1% vs. 1.8%. vs. 1.8%, p=0.69) for inactive, insufficiently active, and sufficiently active individuals respectively. Obesity (BMI >30 kg/m2) was associated with higher prevalence of psychological distress (4.9% vs. 2.9% vs. 2.9%, p<0.01) for obese vs. overweight (BMI 25-25.9) vs. normal weight (BMI 18.5-24.9) individuals. Hypertension was more than twice as prevalent among those with psychological distress compared to those without psychological distress (5.6% vs. 2.7%, p<0.01). Psychological distress was more prevalent among those with hypercholesterolemia compared to those with normal cholesterol (4.7% vs. 2.7%, p<0.01).

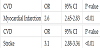
Psychological distress was more prevalent among those with coronary heart disease (CHD) (Table 3) (8.5% vs. 3.4%, p<0.01), for CHD and no-CHD groups respectively. Psychological distress was nearly three times as prevalent among those with stroke (9.8% vs. 3.4%, p<0.01) for stroke and non-stroke population respectively. Chronic kidney disease (CKD) (weak/failing kidney) was associated with four times rate of psychological distress (14.2% vs. 3.4%, p<0.01) for CKD and non-CKD population respectively. Using the logistic regression model, the unadjusted odds ratio (Table 4A) for myocardial infarction in psychologically distressed persons was OR = 2.6 (2.45- 2.83), 95% CI, P <0.01. The unadjusted odds ratio for stroke was OR = 3.1 (2.9-3.3), 95% CI, P <0.01. After adjusting for Age, Body mass index, Diabetes, Hypertension, high cholesterol, smoking, Chronic Kidney Disease, the adjusted OR for myocardial infarction (Table 4B) was 1.96 (1.67-2.3) 95% CI, P<0.01. The adjusted OR for stroke (Table 4C) was 2.5 (2.2-3.0) 95% CI, P<0.01.


4. Discussion
The association between psychological distress, diabetes, hypertension, obesity as well as chronic kidney disease and consequently, CVD could be readily explained by elevated stress hormones that are known to have deleterious health effects. Abdominal obesity, a major risk factor for CVD and metabolic syndrome, is known to be associated with maladaptation to chronic environmental stress which is mediated by a dysregulation of neuroendocrine axes [7]. Chronic activation of the hypothalamic-pituitary-adrenal axis plays a major role in this context together with the stimulation of the sympathetic nervous system leading to chronic diseases including obesity and hypertension [7-10]. While counterregulatory hormones including glucagon, cortisol, growth hormone and catecholamines generally serve as a safeguard to hypoglycemia to counteract the effect of insulin, chronic elevation of these hormones has been shown to be deleterious and is associated with a diabetogenic effect and obesity [11,12]. This concept is readily demonstrable through the high prevalence of diabetes and hypertension in diseases associated with chronic increases in these hormones. For example, high prevalence of diabetes and hypertension is a common feature of Cushing’s disease, which is characterized by chronic elevation of cortisol [13,14]. In patients with chronically high levels of growth hormone, such as those with acromegaly, there is a high prevalence of diabetes and hypertension [15,16]. These disorders are also associated with a high risk of CVD likely explainable by the chronically elevated cortisol in Cushing’s disease [17] and growth hormone in acromegaly [18-20]. These data collectively provide a common soil hypothesis linking psychological distress with the elevated cardiovascular disease risk demonstrated in this study. The data also indicates the role of chronic elevation of stress hormones in the pathogenesis of CVD in adult USA population in this study. Research evidence suggests that atherosclerosis as measured by carotid medial thickness starts as early as adolescence and is linked to urinary free cortisol [21]. High prevalence of psychological distress and CVD among Hispanic and Black populations are readily explainable by the allostatic load caused by adverse socioeconomic factors linked to poverty which lead to worse health outcomes [22-24]. This study also demonstrated a significantly higher rate of psychological distress among women compared to men. This finding is likely a reflection of increased allostatic load among women that has been demonstrated in previous studies [25-27]. Furthermore, chronic activation of the sympathetic system leads to deleterious health effects including elevated blood pressure and blood glucose, and activation of the renin-angiotensinaldosterone system [28-30]. Finally, this study clearly demonstrated not only disparity in the risk factors of CVD among women, racial minorities and socioeconomically disadvantaged by population, but also heightened increase of CVD, the main killer of adult Americans. Effective interventions to treat and manage psychological stress among these vulnerable populations and to eliminate the accompanying healthcare disparities are greatly needed to improve the health, wellbeing and outcomes of CVD.
5. Conclusion
This study demonstrated a relationship between cardiovascular disease (myocardial infarction and stroke) and psychological distress. This association was strong and remained after adjusting for the multiple risk factors of CVD including age, obesity, diabetes, hypertension, dyslipidemia, chronic kidney disease and smoking. These are well-established risk factors for CVD and each of these risk factors are independently associated with psychological distress. This study also demonstrated that psychological distress is strongly associated with adverse sociodemographic factors such as poverty and low educational attainment. Psychological distress was also more prevalent among women and ethnic minorities such as Blacks and Hispanics. Further research is needed to confirm these findings and effective methods for management of psychological distress should be developed and employed in order to decrease cardiovascular disease among the most vulnerable populations.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgments
This work is supported, in part, by the efforts of Dr. Moro O. Salifu MD, MPH, MBA, MACP, Professor and Chairman of Medicine through NIMHD Grant number S21MD012474.