


1. Background
The use of Complementary and Alternative Medicine (CAM) is widespread worldwide especially among patients suffering from chronic diseases including diabetes mellitus. A major reason for the use of CAM is the presence of chronic diseases such as diabetes mellitus [1]. Complementary and alternative medicine is defined as a group of diverse medical and healthcare practices and products that are not generally considered part of conventional Western medicine [2,3]. The plant Galega offcinalis (French lilac or goats rue) is the origin of Metformin which represents the first line in the management of type II diabetes. In the medical literature hundreds of plants have been claimed to be useful for the treatment of diabetes [4]. A recent study of CAM use in people with diabetes demonstrated a huge variation in the prevalence of CAM use across the world from 17% to 73% [5]. However, healthcare professionals need to be vigilant to the possibility of CAM use alongside conventional medicine since fatal interactions have been reported in the literature. Currently, there is a high prevalence of diabetes among the Gulf States coupled with a long tradition of CAM use. A recent study in Saudi Arabia revealed a prevalence of CAM use for the management of diabetes of 30% [4]. A recent study of pregnant females in Qatar found the prevalence of CAM use to be 29% [6]. Qatar is a newly developing country going through a rapid socio-economic transition characterized by a cosmopolitan population with different ethnic backgrounds.
In Eastern culture and in certain ethnicities CAM remedies play an integral part in an individual health belief system, where religious teachings, rituals and family influence play a major role in individual health behavior. Other important components of health self-management include financial resources, culture, and selfempowerment [7,8]. Current data suggest that most patients use CAM in addition to conventional medical treatments [1,9].
However, data is sparse on the types of CAM used by individuals with diabetes. In addition, it is unknown whether individuals with diabetes use CAM more than those with common chronic medical conditions or what factors are associated with CAM use in individuals with diabetes. The aim of this study is to establish the prevalence of CAM use among patients with diabetes mellitus with different backgrounds, religions and ethnicities in Qatar and to explore the characteristics of the CAM users.
2. Methods
2.1 Setting
This is a cross-sectional study of patients registered with Umgwailinah primary health care centre, Doha, Qatar. The authors developed a questionnaire to assess the use of CAM by patients with diabetes over the previous year. Questions were based on the research question and previous similar studies [10]. Questions assessed CAM use in diabetes and whether patients used CAM before their diagnosis of diabetes, classification of CAM, co-administration with medications, information source and the safety and efficacy of CAM. Background information was collected on the respondents' age, educational status, ethnicity, gender, diabetes and self-reported diabetic complications.
2.2 Inclusion and exclusion criteria
All registered patients with type II diabetes above the age of 18 years and a minimum follow-up of one year were eligible for the study. The sample size was calculated using Epi. Info 6.0, based on the prevalence in similar studies, which ranged from (50–56 %) [11,12].
Qatar has an estimated population of 2.5 million with approximately 80% expatriates mainly from the South Asian region. Umgwailinah health centre serves a population which includes approximately 4,500 patients with diabetes. The estimated sample size was 184 with 95% confidence interval and 90% power, and statistical significance level of 5%. The total number of respondents needed was 238, after taking into account a non-respondent rate of 30 per cent. A random sampling method had been used to select participants. The average number of patients with type II diabetes who attend the clinic per day was 30. 460 patients attended in all over four weeks. Since the number of required test subjects was 238, a sampling interval of two was used as the constant difference between subjects. Patients aged less than 18 years and those patients with dementia, any other form of limited understanding or learning difficulty were excluded from the study.
2.3 Data collection
A structured questionnaire was delivered to participants via faceto- face interview after obtaining an informed written consent. The questionnaire was designed to explore patients’ socio-demographic data, co-morbidities, CAM use prior to diagnosis, classification of CAM, types of CAM utilized, resources consulted, safety and efficacy of CAM knowledge, attitude and practice. The main survey was administered during the first four weeks of August 2013 by four healthcare workers.
2.4 Practical definition
A patient with diabetes was defined as someone who was clinically diagnosed with diabetes prior to inclusion in the study or was taking diabetic medications.
CAM therapy was categorized by patients into one of the following six categories: herbal remedies, food supplements, vitamins, homeopathic medicine, natural products and other remedies.
Statistical Package for Social Sciences (SPSS) v. 19.0 was used to analyze the data collected from the study. The findings were described in terms of frequencies, percentages, means and standard deviations. The association between socio-demographic factors (gender, age, race, religion, educational background, occupation, family household income, and duration and control of diabetes) and CAM usage was determined by using Chi-square test. Multivariate logistic regressions were used to identify predictors of CAM usage.
2.5 Ethical approval
Ethical approval was obtained from the Research and Ethics Committee of Hamad Medical Corporation, Doha, Qatar (research protocol #9086).
3. Results
3.1 Socio-demographic characteristics
A total of 238 participants were eligible for inclusion. Ten patients refused to participate in the study. At the conclusion of the study 226 participants had enrolled giving a response rate of 95 per cent. Table 1 shows the socio-demographic information of participants. Participants were mainly females of South-East Asian Muslim origin aged 52–69 years old with a mean age of 45.12 ± 10 years. The majority received tertiary education and the average monthly household income was USD 2,664. The mean duration of diabetes and the mean HbA1c were 7.5 ± 5.7 years and 9.7 ± 1.8 per cent, respectively. The majority of participants (69.9 percent) had underlying hypertension followed by hypercholesterolemia (61.3 per cent), osteoarthritis (6.7 per cent) and asthma (0.9 per cent). The mean systolic and diastolic blood pressures were 148 ± 18 and 85 ± 10 mmHg respectively.

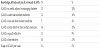
Prevalence of CAM use was 53 per cent. Females were 1.2 times more likely to use CAM compared to males. South-East Asians (60%) were the most frequent users, followed by Iranians (20.8%) and Arabs (19.1%). Table 2 shows CAM use among patients with diabetes. Herbal powder (65%) was the most widely used, followed by Bitter Gourd (54%), Fenugreek (40%), Cinnamon (26%), Ginger (18%) and Coriander (16%).

3.2 Knowledge, attitude and practice towards CAM
Around 19% of participants believed that CAM can be a useful adjunct in the management of diabetes. Thirty per cent of study participants believed that CAM therapies were more effective than modern medicine. 10% considered it equally effective and 25% believed it to be less effective than modern medicine. On the other hand 17.5% of participants believed CAM to be safer than modern medicine, 10.0% considered it equally safe and 4.0% of the participants found it to be less safe than modern medicine.
Some used it because they are following the example of other CAM users (17.3 per cent) (Table 3).
3.3 Sources of information about CAM
Our data found that participants learned about CAM from family members (42.1 per cent), friends (23.8 per cent) and the media (12.4 per cent). The mean duration of CAM usage was 5.0 ± 3.6 years. The mean frequency of consumption was 3.1 times per week.
3.4 Multivariate logistic regression
Table 4 summarizes the characteristic differences between CAM users and non-CAM users. A calculation was carried out to explain the results of unadjusted univariate logistic regression analysis of variables related to CAM users. A multivariate logistic regression analysis was used to independently predict a (CAM) user after adjustment for variables that attained P < 0.05 in univariate analysis and clinical significant variables. Being South East Asian (odds ratio [OR] 5.297, 95 %, CI 2.892-9.377), Muslim (OR5.259, 95%, CI 2.995-9.198) and attaining a secondary and higher education (OR 5.239, 95%, CI 2.898-9.595) were the only predictors for (CAM) use after adjustments for gender, ethnicity, religion, occupation, family household income and hypertension.

4. Discussion
Our data highlighted a common practice among Patients with diabetes in Qatar. To the best of our knowledge this is the first study of its kind performed in Qatar to assess the use CAM remedies among patients with diabetes on conventional treatment. The study specifically focused on non-commercially available types of CAM used by diabetics as supplements to daily food intake.
The prevalence of CAM usage among DM patients in this study population was high (53 per cent). This is consistent with findings in other studies [9]. However, this may be under-reported since many patients may feel embarrassed about divulging information in regards to CAM use whereas others may use different types of CAM that are not specified in the study definition. Patients may also consider these products part of the normal diet - especially among ethnic minorities.
- Patients with diabetes may opt for CAM therapies for a variety of reasons including the high cost of modern medicine, fear of hypoglycaemia associated with oral hypoglycaemic medications, the large amount of tablets taken, frustration with uncontrolled diabetes, risk taking behaviour and the belief that herbal treatment is safe since it comes from nature. Other factors which may influence CAM consumption among patients with diabetes include strong media campaigns, high availability, peer pressure, family influence and religious teachings. The Quran for instance hails honey for its healing properties "Your Lord revealed to the bees: "Build dwellings in the mountains and the trees, and also in the structures which men erect. Then eat from every kind of fruit and travel the paths of your Lord, which have been made easy for you to follow." From inside them comes a drink of varying colours, containing healing for mankind. There is certainly a Sign in that for people who reflect" (The Holy Quran 16: 68) [13].
and many herbal products are already mentioned in the Holy Quran including onions, garlic, olives, figs and lentils. Muslims are influenced by the teachings and content of the Quran thereby their attitude towards herbal remedies is reinforced. South-East Asians on the other hand tend to use herbal remedies for a variety of reasons including cultural factors, preferences to be treated holistically and the increased availability of CAM [14,15].
In this study, 30% of respondents thought that CAM was more effective than conventional medicine, 19.1% thought of CAM as a useful adjunct in managing diabetes and 17.5% thought of CAM as safer than conventional medicine. This is in contrast to a US-based study that reported “users of alternative health care are no more dissatisfied with or distrustful of the conventional care than nonusers are” [15]. One possible reason for this study’s findings is that most CAM users had poor glycemic control and because health professionals usually stress to their clients to adhere to diet, change of lifestyle, and behaviour [16,17]. As a coping strategy patients may revert to CAM therapies in the hope that they may improve their glycemic control and avoid injectable insulin. On the other hand, it could be related to underlying shared beliefs and cultural assumptions [18], especially among Muslim patients where the Quran has explicitly spoken of the benefits of herbs and natural honey.
In the present study, the main variety of CAM used were herbal powder (54%), along with bitter gourd (44%), fenugreek(40%) and cinnamon (26%). These findings are not surprising, since most respondents believed that herbs are safer, more effective than conventional medicine and are a useful adjunct. These findings are consistent with studies done elsewhere on ethnic populations [19,20]. Participants learned about CAM primarily from family (42.1 %), friends (23.8%) and the media (12.4%). These findings should prompt health care professionals to consider involving family members and friends during educational sessions in order to explore the use of CAM in diabetes management.
Qatar is a cosmopolitan, multi-ethnic, multi-cultural, multireligious newly developing countries in which South-East Asians form the majority - constituting 45% of the population [21]. In this study South-East Asian patients were more likely to consume CAM compared to other ethnicities (P 0.001). Among South-East Asians CAM use is deeply embedded and influenced by religious and cultural factors. Use of herbs like bitter gourd, cinnamon and fenugreek are believed to reduce blood sugar levels [22,23,24]. Bitter gourd is the most common herb used by South-East Asians since before the 15th century [25].
Belief in Islam was found to be one of the strongest predictors for pursuing CAM therapy (P 0.001). One explanation for this may be that CAM usage has always been embedded into the Muslim belief system and cultural heritage that is already deeply integrated into their lives [26,27].
Similar to studies elsewhere [28-30], our data shows that patients with higher levels of education were more likely to be CAM users. However, this study found no significant relationship between CAM usage and age, gender, household income, co-morbidities, type of work and HbA1c level.
Patients with diabetes are more likely to resort to CAM therapies - regardless of gender or socio-economic status according to a U.S. based study that reported that patients with diabetes were 1.6 times more likely to use CAM than their non- diabetic counterpart [31].
Glycemic control in this study was not influenced by the use of CAM. This could be explained by lack of exercise and embracing a westernized life style coupled with sedentary types of jobs and hot and humid weather for around eight months of the year. All these factors preclude patients from embarking on physical activities along with a negative attitude towards exercise [32]. When educating patients on CAM use, health care workers should respect patients' choices while providing evidence-based information about efficacy and safety or the lack thereof.
5. Strength and Limitations
Time constraints have precluded us from including a non-diabetic group as the control group in this study. Although it is prudent to evaluate the prevalence of CAM use in patients with diabetes via a randomized representative sample, this option was not viable as Qatar like other countries in the region lacks a national diabetes registry. The lack of measurement of hypoglycemia, based on a symptom score or an objective biochemical measure is identified as a limitation in this study, which should be addressed in subsequent studies. The inclusion of South-East Asians in this study is important since they form the majority ethnic group in Qatar and no such studies were carried out in this part of the world.
6. Conclusion
There is a high rate of CAM use in patients with diabetes attending primary health care clinics in Qatar. The high prevalence rate of CAM use should prompt clinicians to further explore this topic with their patients in order to manage diabetes accordingly and be aware of the serious interaction between herbal and classical medicine. This is important since most patients do not divulge this information to their physicians.
Competing Interests
The authors declare that they have no competing interests.
Abbreviations
CAM: Complementary and alternative medicine
BP: Blood pressure
DM: Diabetes mellitus
SPSS: Statistical package for social sciences
HbA1C: Glycosylated haemoglobin
USD: United States dollar
OR: Odds ratio
CI: Confidence interval.