


1. Introduction
Asthma inflames and narrows the airway to cause shortness of breath, cough, wheeze, and chest tightness that can affect people irrespective of their age [1]. Evidence suggest that in Oman about 7.3% adults and 12.7% of children are prevalent with asthma and 95% of them avails the government healthcare facilities. Inpatient services are utilized by the major population (55%) followed by emergency (25%) and outpatient visits (20%) [2]. Recent facts on asthma in the region also indicate a low level of asthma control placing a large economic burden on health care sector [3].
Public health care system and clinicians rely on health-related quality of life (HRQoL) and well-being assessments for chronic diseases like asthma to find its impact on physical, mental, social and societal functioning [4]. HRQoL measurements are also important in determining the value of drug treatments in chronic conditions [5].
Asthma control is a predictor of disease-specific quality of life and is associated with significant impairment in the health status of the patients even with differences in severity. Hence various treatment focuses is to attain the best possible control over asthma regardless of initial severity [6]. The burden of asthma is complex among midlife adults and the elderly population who might have a co-occurrence of chronic obstructive pulmonary disease (COPD), a worsening factor in asthma control [7,8]. According to current guidelines, the longterm goal of asthma management includes good symptom control and reduction in exacerbations and limited side effects of treatments. Control-based management strategies incorporate continuous assessment, treatment and review of patient response with respect to above goals [9].
Ambulatory cares for asthmatics are limited to mild and moderate persistent patients when compared to severe persistent asthmatics. This often decreases the need for emergency department visits and inpatient admissions due to asthma exacerbations. Population studies to evaluate the quality of life and asthma control among people in Oman are inadequate, projecting to a lack of data to understand the influence of disease severity and what existing inconsistencies in ambulatory care for mild to moderate asthma patients.
2. Methodology
The prospective study was conducted on 31 asthma patients who were categorized as mild to moderate severity based on GINA (Global Initiative on Asthma) [9] categorization. The patients enrolled received ambulatory care for asthma at the secondary care hospital run by the Ministry of Health, Oman. Asthma patients received medications like inhaled corticosteroids and beta 2 agonists for a period of six months with monthly follow-ups. Salbutamol was given as and when required for all the patients. Majority of patients used metered dose inhalers (MDI), few dry powder devices (diskhaler) and the inhaler techniques were reassessed during each follow-up.
Patients satisfying study criteria signed an informed consent to enter the study. Pregnant patients and those with severe asthma requiring hospital admissions or comorbid conditions like ischemic heart disease and congestive cardiac failure were excluded. Peak expiratory flow rate was checked during the visits to assess the severity of disease for patients in the study. The demographic details included all basic information such as age, sex, education level, duration of disease, occupation, family history, social history (alcoholism and smoking history) medication received history of atopy and other comorbid conditions. History of bronchodilator usage in the previous week was also recorded.
Asthma quality of life was assessed using Mini Asthma Quality of Life Questionnaire (Mini-AQLQ), a disease-specific 15-item selfadministered questionnaire developed and validated to measure functional impairments in 4 domains: symptoms, activity limitation, emotional function, and environmental stimuli. Patients were asked to recollect their experience during preceding weeks and answer each question on a 7-point scale (7=no impairment, 1=severe impairment). It is a condensed version of 32-item Standardized Asthma Quality of Life Questionnaire (AQLQ-S) which consumes only 3 to 5 min to complete. A clinically relevant minimum difference is 0.5 and the scores less than six shows a significant impact on QoL [10].
2.1 Statistical analysis
The results were analyzed using SPSS version-20. Descriptive statistics were performed to project data with frequencies, mean and standard deviation. Descriptive statistics applied for demographics and data presented in percentages and mean ± standard deviation. Independent sample t-test was performed to the severity subgroups of Mini-AQLQ scores and ACT values. Pearsons correlation was done to establish an association of ACT to AQLQ total score. A p-value<0.05 was considered for a statistically significant difference.
2.2 Ethics
The study was approved by the regional research and ethics committee of the Ministry of Health, Al Dhakhiliya Governorate, Sultanate of Oman.
3. Results
The study patients were majority of females (74%) and about 74.2% of the patients were having moderate persistent asthma according to GINA classification. Allergic rhinitis was very common among 61.3% of patients with asthma. The asthma control test scores revealed that 58% of patients scored 19 and above indicating good control over their asthma and the average ACT score was 22.5±1.64. The 4 weeks history of asthma problems were troublesome and needed greater levels of rescue inhaler support for the remaining 42% showing a lesser than 19 ACT scores. The majority (45.2%) of asthma patients were in the age range of 18 to 28 years and lesser (19.4%) in age above 48 years. Demographic characteristics with the percentage of patients are shown in table 1.

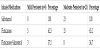
Overall the patients had an average age of 34.16±12.42 years with good control over asthma with an average ACT scores 22.5±1.64. The lung functions were assessed using the peak expiratory flow rate (PEFR) meter for every patient during the ambulatory care. The PEFR percentage predicted was found to be 72.74% indicating mild to moderate persistent asthma. The overall quality of life (QoL) among asthma patients showed a decline with an average score of 3.99±0.87. However, the overall symptoms scores were showing the best result of 4.89±1.26 for asthmatics under study. The total score of AQLQ was similar among female patients (3.99±0.96) compared to male (3.98±0.6) indicating that no sex wise difference in the quality of life observed among the patients. The basic parameters of asthma control, lung functions and quality of life asthma patients are shown in table 2.

The asthma medications were given to patients based on the severity of disease according to Ministry of Health guidelines. All patients received as required Salbutamol inhaler and continuous fluticasone inhaler. Whereas, a combination of fluticasone and salmeterol was received by a small group of both mild (37.5%) and moderate (34.7%) categories of patients. The medication use among the asthma patients in the secondary care hospital is shown in table 3.
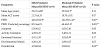
It was observed that patients with mild persistent asthma were of lesser age (29.13 ±4.86) range compared to moderate persistent cases (35.91±2.5). The lung functions recorded using PEFR values among the mild and moderate persistent patients shown a high level of significant difference (p<0.05) indicating the need for further closer management of the disease. This was also reflected in the domain scores of Mini-AQLQ.
Though the domain scores of mild and moderate asthma groups have shown wider differences in scores between them, there was no statistical significance (p>0.05). The moderate persistent asthmatics reported a poor quality of life (3.8±0.81) compared to patients with mild persistent asthma (4.53±0.84). Moreover, the overall quality of life represented by AQLQ total scores have shown a significant (p=0.03) difference in QoL. The subgroup data analysis comparing mild and moderate persistent asthma patients is shown in table 4.
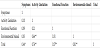
The association between asthma control and health-related quality of life was conducted using a 2-tailed Pearson’s correlation model. It was observed that the overall quality of life correlated (0.48) well with asthma control and its association was highly significant (p=0.01). However, the emotional function has shown the poorest association (0.09) among overall patients and a negative association (-0.17) among moderate persistent asthmatics.
The subgroup analysis has shown a significant association between activity limitations even with the asthma control among moderate persistent asthma. This indicates the need for rechecking the antiinflammatory control over this category of patients. The relationship between quality of life and asthma control is represented in table 5.

The quality of life variables of AQLQ has shown significant associations between its domains. This indicates the close relationship of AQLQ variables to explain the quality of life in asthma patients. Furthermore, it indicates the appropriateness of this instrument in evaluating QoL among Omani populations. It was noted that each individual domains of Mini-AQLQ significantly correlates with the overall quality of life (total scores) of asthmatics among the population. The association of activity scores (0.76), emotional functions scores (0.57) and environmental stimuli scores (0.81) were highly significant (p=0.01). The AQLQ domains relation with overall QoL in asthma patients is shown in table 6.
4. Discussion
The major findings of this study conducted at Sultanate of Oman using Mini-AQLQ observe a decline in overall health-related quality of life among mild to moderate persistent asthma patients treated at the secondary care hospital. In Oman, the majority of asthma patients have been treated at the ministry of health, primary and secondary care hospitals and are getting the paramount treatment.
The study findings proved that quality of life is interrelated with asthma control and its association was highly significant among the Omani population. A highly significant correlation was observed between total AQLQ score and ACT scores. Yet, the emotional function has shown the poorest association among all the patients and a negative association among moderate persistent asthmatics.
Moreover, this correlation was not significant with the emotional functions and also symptoms. Other studies have shown similar findings, where the total AQLQ score was highly correlating with ACT for all four domains like symptoms, activity, emotional and environmental [10]. These outcomes are in-par to studies conducted in Saudi where all the other quality of life aspects correlated well with asthma control except the emotional functions [11]. Studies reported that a single point increase in ACT scores is related to an increase in 0.129 points in AQLQ [12]. This was highly supported by the study findings conducted in the Omani population showing highly significant positive correlations among AQLQ and ACT scores.
The quality of life was incomparable among both sexes even though more female patients were in the study. Though less in number, the male patients experienced a lesser quality of life could be the reason behind the same. This is in contrary to other studies conducted in Iran and Saudi where the female patients had lesser QoL compared to male patients [12,14,15].
Comorbidities could be another reason to justify this problem. Most of the male patients were suffering from comorbidities like diabetes and allergic rhinitis along with moderate persistent asthma. Studies reported that lower QoL is experienced among patients, who had admissions due to chronic diseases like diabetes [14].
The study findings suggest that the activity limitations and environmental stimuli are unavoidable factors to be addressed for the control of asthma. This, in turn, influences the quality of life of patients. A positive correlation to these factors highlights that asthma control among Omani population. The environmental stimuli like sandstorms in some areas of the country and even personally the use of incense burners at home all are accountable for patients who are living with triggers.
Only PEFR reading was available to assess the lung functions. In general, the primary and secondary care setups hardly perform lung function assessments using spirometer for checking FEV1 and FVC. However, most ambulatory care clinics use peak flow meters to measure the PEFR values and the percent predicted values were used to assess the severity of patients. This may be due to the unavailability of technicians or trained staff to perform the assessments and requires a certain time and sufficient room for the respiratory physicians with the number of outpatients. Pharmacist-led Asthma clinics are now becoming a greater support to the medical team by assisting in spirometric evaluations along with the pharmaceutical care aspects.
The lung functions using PEFR percentage predicted was indicating mild persistent asthma among overall patients and the total QoL declined (less than 6 scores). These findings are similar to studies conducted in other middle-east countries where the AQLQ scores reflect poor quality of life with less than 6 scores on AQLQ [12,15].
The subgroup analysis has shown a significant association between activity limitations even with the asthma control among moderate persistent asthma. Moreover, the PEFR values among mild and moderate persistent patients also shown significant difference indicating the need to recheck the anti-inflammatory treatment given to patients particularly in GINA-3. Inhaled corticosteroids were received by all asthma patients but were restricted to the drug fluticasone alone as inhaled corticosteroid medication.
A combination of fluticasone and salmeterol was received by a smaller group of both mild and moderate persistent asthma patients. The treatment of GINA-3 (moderate persistent) asthma patients in secondary care setups need to be more standardized based on the GINA guidelines with the support of spirometric evaluations. If ignored, would further lead to poor quality of life and the long-term sufferings due to airway remodeling [16]. Inspite of the availability of current treatments in managing asthma, phenotypes are being considered to personalize asthma treatment in uncontrolled severe asthma provided all other confounding factors like poor dosage regimen, inhaler technique, poor adherence, comorbidities, and modifiable risk factors are excluded [17].
Mini-AQLQ is an appropriate instrument in evaluating QoL among Omani populations. The specific domains of Mini-AQLQ significantly correlate well with the overall quality of life of asthmatics among the population. The activity scores, emotional functions scores and environmental stimuli scores were significantly correlating. Hence, the QoL instrument Mini-AQLQ is well suitable for use among Omani population.
The major limitation of the study is lack of spirometry data for correlating asthma control and quality of life. The number of patients in mild persistent asthma was lesser for any comparison.
5. Conclusion
Moderate persistent asthma patients experienced poor quality of life and need modification in anti-inflammatory treatment using inhaled medications. Mini-AQLQ is adaptable in Omani population for QoL evaluation. The activity limitations and environmental stimuli are unavoidable factors to be addressed for the control of asthma among Omani population to achieve a better quality of life.
Competing Interests
The authors declare that they have no competing interests.