


1. Introduction
Puerperal infections/sepsis is a major public health and historically considered as a common pregnancy-related condition, which could eventually lead to obstetric shock or even death. It is a preventable disease which occurs within six weeks of giving birth [1] . According to the World Health Organization (WHO), puerperal infections/ sepsis is the sixth-leading cause of deaths among new mothers while it contributes 15% of total maternal deaths globally among the mothers of the reproductive age [2] . The global incidence of puerperal sepsis is 4.4 per 100 live births [3] . According to the WHO, proportion of maternal deaths due to puerperal sepsis are 9.7%, 11.6% and 7.7% in Africa, Asia and Latin America and the Caribbean respectively. On the other hand puerperal sepsis contributes only 2.2% of maternal mortality in developed countries. The Odds Ratios are 2.71, 1.91 and 2.06 in Africa, Asia and Latin America and the Caribbean respectively comparing to the developed world [4] . It is found as one of the leading cause of maternal deaths in the intensive care unit in the USA [5] . In Nigeria, puerperal sepsis is the 3rd leading cause of maternal mortality and contributes 12% of maternal mortality [6] . The incidence of puerperal sepsis in different African countries are 1.7, 0.22, 1.14 and 0.07 per 100 live births in Nigeria, Niger, Uganda and South Africa respectively [7] . Several studies from Pakistan established puerperal sepsis as the 3rd leading cause of maternal mortality [8] and the incidence is 10-15 per 100 live births [9] . Another study from Pakistan also identified 13 to 16% of all maternal deaths occurred in the post-partum period and puerperal sepsis contributed 12.4% of those deaths [10] . A study from Senegal demonstrated an incidence of sepsis of 8.7 per 100 live births for home deliveries compared to 1.9 per 100 live births for deliveries in health facilities [11] .
In Bangladesh, information on puerperal sepsis is limited due to socio-cultural behavior related to health care seeking pattern of the pregnant women. However, available data shows that the incidence of puerperal sepsis in Bangladesh is 4.5 per 100 live births [6] . Two hospital-based studies conducted in Mymensingh Medical College Hospital and Dhaka Medical Collage Hospital in Bangladesh revealed that maternal mortality due to puerperal sepsis in these two government health facilities was 17 and 20.3 per 100 live births respectively [12,13]. A community survey in a Dhaka slum reported that more than three-quarters of women suffered from a non-trivial illness during the first 6 weeks postpartum [14] .
Literatures established that the predisposing factors for puerperal sepsis includes; anemia in pregnancy, prolonged labor, frequent vaginal examination, premature rupture of membranes and use of unsterilized/unwashed instruments during delivery [15] . Morbidities associated with puerperal sepsis includes; fever greater than 38.0°C (100.4°F), chills, vaginal discharge, septicemia, peritonitis or abscess formation leading to surgery, endo-toxic shock, pelvic abscess, and finally mortality among others16,17. Ensuring healthy lives and promoting the well-being for all at all ages is essential to sustainable development. As part of the sustainable development goals (SDGs) it has been targeted to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by 2030. Though Bangladesh has made success in reducing maternal mortality significantly but to achive the target 3 of SDGs it is crucial to address maternal mortality due to puerperal sepsis. Reliable data on the determinants of puerperal sepsis is essential to improve post-partum health care services which is largely unavailable in Bangladesh. Hence, our study aimed at exploring the socio-demographic determinants of puerperal sepsis in tertiary level government health facilities.
2. Method
A case control study was carried out during April and December 2011 in two tertiary level government health care facilities/hospitals in Dhaka city to identify the socio demographic and economic risk factors of puerperal sepsis. Respondents were selected purposively as it is relative ease with which sample units can be selected. A total of 140 female respondents/participants (35 cases and 105 controls) were selected for this study. Female with puerperal sepsis were considered as the cases while mothers who were admitted in the same health care facilities (hospitals) during the same period were recruited as controls. Controls were the mothers who had childbirth at least 42 days before hospitalization with other conditions. Patient with multiple complications such as obstetrical fistula, patient with the state of immune suppression for example HIV/AIDS and patients with the systematic infections such as TB were excluded from the study. An informed verbal consent was taken from the participants before interview.
A structured questionnaire was developed through a national workshop with the subject specialist and key stakeholders. The drafted questionnaire was pre-tested and adjusted according to the feedback from pre-testing before actual data collection. Main investigator of the study personally collected data to ensure quality of data.
The investigators of the study developed a program to enter data using Epi-Info 6 software. Data were double entered and matched later as part of the quality control mechanism during data entry. Data were transferred into SPSS 20 to carry out all the statistical analysis. Descriptive analysis was performed including frequency distributions and calculation of means and standard deviation for continuous variable. Odds Ratio was calculated at the 95% Confidence Interval for each variable to find the potential risks. Chi-square test was performed to understand the associations between the dependent and the independent variables. Logistic regression analysis was also performed to find out the association between independent and dependent variables. The study followed the guidelines of ethical consideration of the Bangladesh Medical Research Council (BMRC).
2.1 Operational definition
2.1.1 Puerperal sepsis
Infection in genital tract which occur at any time between the rupture of membranes or labor and the 42nd days of post-partum in which 2 or more of the mentioned symptoms are present is called puerperal sepsis. Symptoms are pelvic pains, fever (that is oral temperature 38.5°C or higher) on any occasion, abnormal vaginal damage (example presence of pus) abnormal smell or foul odor of discharge, delay in the rate of reduction of the size of the uterus (less than 2 cm per day during the first 8 days) [16] .
3. Results
Over the study period 35 patients were diagnosed with puerperal sepsis by the clinician according to history, symptoms and signs who were recruited as cases. 105 mothers from the same hospitals were also recruited as controls. Table 1 shows the socio-demographic and economic data of the respondents.
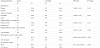
The mean maternal age of the respondents was 27 years (SD±4.58). Out of 140 respondents, 25% (n=35) were cases and 75% (n=105) were controls. Figure 1 shows that the proportion of mother less than 25 years was more among the cases (71.4%) compare to controls (32.4%). Puerperal sepsis was significantly associated with <25 years age group compared to > 25 years (OR = 5.22; 95% CI: 2.25-12.08; p= <0.001).

A large proportion of puerperal sepsis cases were from the urban areas (68.6%) compare to the rural areas (31.4%). However, no significant association between the occurrence of puerperal sepsis and the area of leaving (OR= 0.56; 95% CI: 0.25-1.27; p= 0.16) was found. Among the cases 65.7% were from the joint families while 52.4% of controls were from nuclear family. But it did not differ significantly between the groups (OR= 0.47; 95% CI: 0.21-1.05; p= 0.63). No significant association between the occupation of the respondents and development of puerperal sepsis was established. Unemployed respondents mostly comprised of housewives in both cases (74.3%) and controls (84.8%). Only few respondents were employed (25.7% of cases and 15.2% of controls). Unemployment was not likely to increase the chances of developing puerperal sepsis (OR= 0.51, 95% CI: 0.51– 1.31; p= 0.16).
Among the cases, 62.9% had below secondary level education while 67.6% of controls had above secondary level education. However, in multivariate logistic regressions analysis no significant association between development of puerperal sepsis and respondents’ education was found (Table 2). But when education of husbands were assessed, a significant association was found. A large proportion of husbands of the cases (97.1%) had below secondary level education compared to controls (23.8%) (OR= 108.80, 95% CI 14.16- 835.61; p =0.00). Figure 2 shows that 85.7% of cases came from poor economic status compare to 16.2% of the controls. Poor economic condition was found significantly associated with development of puerperal sepsis (OR= 31.0, 95% CI 10.5-91.4; p =0.00).


4. Discussion
In the study it was revealed that women becoming pregnant before 25 years of age had a significant association of developing puerperal sepsis which is quite similar with a study conducted in Egypt which shows that 71.4% of cases were <25 years old comparing 32.4% among the controls [18] . Similar findings have been found in another study from Nigeria where they identified that the maternal age below 24 years is associated with puerperal sepsis with an OR 1.32 [19] . A study from Hyderabad also identified that 67.2% of the mother who developed puerperal sepsis were below 30 years of age [20] . Probably, the reason of such finding is physical vulnerability of inexperienced young mother.
In our study, we did not find any geographical variation especially between rural and urban settings in developing puerperal sepsis. However, few studies conducted in other parts of the world found a positive association between area of living and puerperal sepsis. A study from Pakistan identified that 86% puerperal sepsis cases were from the rural areas compared to 13% from the urban areas [20] . The reason is that in rural areas women did not receive any kind of antenatal and post-natal care and most of the delivery took place at home by the untrained birth attendant.
In our study, there was an association between development of puerperal sepsis and lack of education of the respondents. 62.9% of cases had below secondary level education while 67.6% pf controls had more than secondary level education. Similar findings have been revealed in a study where it was found that 96% women were uneducated and only the rest had below primary level of education who developed puerperal sepsis [21] . Another study from Karachi found that almost two thirds of the women having puerperal sepsis did not have any formal education, 21.4% had 1-5 years of formal schooling, 9.5% had 6-10 years of formal schooling and only 7.6% had more than 11 years of schooling [22] .
A strong association between the development of puerperal sepsis in women and education of their husband was found in the study. In the study it is found that 97.1% husband among the cases had below secondary level education compared to 67.6% husbands among the controls having the same level of education. Only few studies measured husbands’ education with the development of puerperal sepsis among women. A descriptive study conducted in Liaquat University Hospital identified that 50% of the husbands were uneducated and 50% had eight years of schooling among the puerperal sepsis patients [20] .
Total family income represents the socio economic status of the respondents. Our study found that puerperal sepsis was significantly higher among the mothers of lower socio-economic status. Less than 15,000 taka monthly family income is counted as low socio economic status in our study. We have identified that 97.1% cases were from lower socio-economic status compared to 46.7% of the controls were from the same economic group. Similar findings have been identified in several studies. A study from Pakistan found that 67.2% patients with puerperal sepsis came from the low socio-economic status [20]. Study conducted in Zambia identified that low socio-economic status is a risk factor for developing puerperal sepsis [23] and another study from Alexandria also found that low socio-economic status (OR: 6.4) is a predesposing factor for puerperal sepsis18. The reason of getting higher chance of puerperal sepsis among the poor class people are chronic ill health and malnutrition which is common among low socio-economic profile females [24] . The women of Bangladesh are not only disadvantaged by economic and social condition but also having limited access to adequate health care services. Around 77% population of Bangladesh live in the rural areas. Out of which 60% are living under the poverty level and poor people cannot effort the proper or standard heath care services, thus the women of this economic strata deliver their babies in the unhygienic condition [25] .
To interpret the results of this study, we must explain its limitation as well as its strength. The strength of the study is that it was conducted in tertiary care hospitals where patients from all socio-economic class came. There were three (3) controls recruited for every case which gave the study strength. Though the study found important findings but it has several limitations as well. Firstly, the study had to rely on the hospital patients. The findings may not represent the true burden of the disease in the community as many women with puerperal sepsis may not get the access to the health care facilities for many reasons: geographical distance, financial constraints, and cultural beliefs – sometimes they have to ask permission from their husbands to go to hospital. Another problem may be that most postpartum infections take place after hospital discharge, which is usually 24 hours after delivery. Therefore, in the absence of post-natal follow-up many cases of puerperal infections can go undiagnosed and unreported. In our study we could not do such follow-up during the post-partum period due to time limitation and distance. Finally, several social determinants of puerperal sepsis could not examined due to small sample size.
5. Conclusion
Puerperal sepsis is a common public health problem that contributes a lot in the maternal mortality and morbidity in Bangladesh; ultimately have an impact in achieving the target 3 of sustainable development goals. Findings of this study could be an insight for the policy makers in addressing the burden of puerperal sepsis through a holistic approach in combination of improving post-natal followup and raising community awareness. We suggest that early child bearing should be discouraged along with education up to secondary level should be free by the government. Further community-based research including national prospective to evaluate the magnitude of the puerperal sepsis and find out the risk factors is recommended.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
All the authors have substantial contributions for the paper. TT was responsible for field level data collection, data analysis and drafting the first manuscript, SM, IT, KNA and CSM was responsible in finalizing the methodology for the study, supporting the 1st author in analyzing the data and reviewing the manuscript for necessary correction and improvement.