


1. Introduction
Type 2 diabetes (T2D) in children and adolescents is emerging as a health problem worldwide due to the global epidemic of obesity, accounting for as many as 46% of new cases in Latin populations [1]. In the majority of these cases, chronic complications can be detected since its diagnosis, such as hypertension, nephropathy, neuropathy or dyslipidemia [2]. Hepatic steatosis (HS) and non-alcoholic steatohepatitis (NASH), is seldom searched for in these patients, although it has been reported in up to 78% of adults with T2D [3] and it is considered the most common liver pathology in adults and children [4].
The gold-standard for the diagnosis of HS is liver biopsy, but this is a costly procedure that is not exempt of possible severe complications. This is why, in the last decade many other non-invasive diagnostic methods have been used instead. Some imaging modalities include ultrasound, computed tomography or magnetic resonance imaging, have been used with excellent results [5]. The hepatic ultrasound has reported a 100% sensitivity in detecting more than 33% liver fat and a positive predictive value of 62%. Other authors have used different serum markers and biochemical scales to diagnosis HS, such as the SteatoTest and fatty liver index [6].
RBP4 is a member of the lipocalin family of proteins with 201 amino acids. It is mainly expressed in liver and adipose tissue, and it transports retinol and binds to transthyretin, which prevents its renal excretion [7]. Studies in humans have linked this molecule with obesity and insulin resistant (IR) states, such as the metabolic syndrome (MS) or T2D [8]. Its also been associated with increased levels of visceral fat [9]. In pediatric population, RBP4 is elevated in obese patients, and it showed a positive correlation with body mass index (BMI), higher visceral fat, different components of the MS and some serum markers of systemic inflammation [10]. In recent years, the relationship between this molecule and HS has been evaluated, finding positive correlations with increased liver enzymes in several studies [11]. RBP4 levels are also increased in, obese and non obese T2D patients, compared with non-diabetic weight matched controls [12,13].
There is scarce information with regard to the presence of HS in T2D in pediatric population, and to the expression of this adipcytokine in these patients. The aim of this study was to identify the frequency of HS in T2D children and adolescents and evaluate the RBP4 serum levels, and its relationship to HS.
2. Materials & Method
A cross sectional study was conducted in 34 T2D children and adolescents aged 8 –18 years attending the outpatient diabetic clinic at the Hospital Infantil de Mexico Federico Gomez (Mexico City, Mexico). All patients were diagnosed according to the American Diabetes Association criteria [14,15], and were on multiple dose dietary treatment according to age, BMI and Tanner stage and either metformin (41%) or insulin (24%), or a combination of both (35%). Exclusion criteria were evidence of thyroid dysfunction, hepatic, renal or liver disease, chronic or acute infections, micro or macrovascular complications. The patients were divided into 3 groups according to the degree of HS on ultrasound for their analysis: No HS (NHS) (n=13), mild HS (MHS) (n=15) and severe HS (SHS) (n=6) patients. Parental informed written consent and child assent were obtained from all participants. The protocol was approved by the Institutional Review Board of the Hospital Infantil de Mexico Federico Gomez.
3. Measurements
All patients with help from their parents completed a brief questionnaire regarding age, sex, age at diagnosis, pharmacologic treatment and presence of complications or other diseases. Weight, height, body mass index (BMI), waist circumference, blood pressure and Tanner stage was evaluated by a trained pediatric endocrinologist. A blood sample was taken, after an overnight fast, to determine glucose, glycosilated hemoglobin A1c (HbA1c), total cholesterol, high density lipoprotein cholesterol (HDL-c), low density lipoprotein cholesterol (LDL-c), triglycerides, hepatic enzymes (ALT, AST and GGT) and RBP4 levels.
Serum glucose, ALT, AST and GGT concentrations as well as HbA1c, total cholesterol, HDL-c and triglycerides were measured with the Siemens Dimension RXLMAX System (Siemens Healthcare Diagnostics). The LDL-c levels were calculated using the Friedewald formula modified by De Long. RBP4 levels were measured by ELISA (Millipore Linco-Research kit). Coefficient of variation for this determination was 7.7%.
To evaluate the presence of HS, an hepatic Doppler ultrasound (Siemens, 5.5Hz) was performed to all patients by a trained pediatric radiologist, taking into consideration 3 aspects to determine the degree of hepatic steatosis: 1) echo levels of liver and kidney parenchyma, 2) echo penetration into liver (diaphragm visibility) and 3) clarity of liver blood vessel structures (veins) [modified form Tominaga 1995] [ 16]. Each of these was given a value from 0 to 3, zero being of normal characteristics, and 3 being completely abnormal. The 3 values were added and the degree of HS was determined by the total score in this manner: 0: NHS, 1-3:MHS and >4:SHS, and thus patients categorized into the 3 different groups.
4. Data Analyses
Data are expressed as mean ± SD or median (maximum and minimum value) if the data were skewed distributed. Statistical analyses were performed using analysis of variance or Kruskall Wallis test for comparison. Pearson correlation test was used to examine relationships between variables. All analyses were conducted using the Stata SE V. 11. All p-values≤0.05 were considered statistically significant.
5. Results and Discussion
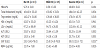
Clinical and antrophometric features of the 3 groups are depicted in Table 1. No differences were found between the 3 groups in age, age at diagnosis, weight, height, BMI waist circumference (WC), blood pressure and Tanner stage.

With regards to the level of disease control, the HbA1c levels and lipid profile were similar between the 3 groups (p>0.05). There were a significant increase in the levels of ALT and AST in the SHS (p=0.002 and p=0.001 respectively). The levels of GGT did not have a statistical difference, but the level in patients with SHS was twice as high as the other 2 groups (Table 2). RBP4 levels were also higher in the SHS group (p=0.04). RBP4 showed a positive correlation with HS (r=0.487, p=0.043) and ALT levels (r=0.367, p=0.035). Table 3.

The prevalence of HS in T2D adult patients varies widely, ranging from 21 to 78%, and the presence of diabetes is a strong independent predictor of progression to fibrosis [17]. There are very few reports concerning to the presence of this disease in children and adolescents with T2D. Dean and Sellers [18] studied 49 patients, from 8 to 18 years of age, and reported that 44% had elevation in ALT, AST or both. Nadeau, et al [19] reported elevation in ALT in 48% of 115 adolescent patients with T2D. In our study the frequency of HS was 61%, with 17% showing signs of SHS in the ultrasound. Only 20% had high levels of ALT, and non were higher than twice the normal value. This data shows the presence of HS in many patients with normal levels of liver enzymes, and could indicate the need for an earlier detection, either by ultrasound or with some other serum marker, to avoid the progression to steatohepatitis.
In our study we found that RBP4 correlates with the degree of HS in children and adolescents with T2D. These results are in agreement to those published by Romanowska, et al [13], who found elevation of this adipocytokine in obese pediatric patients with NASH compared with normal weight controls, and who also found a positive correlation between RBP4 levels and degree of HS by ultrasound (r=0.45;P=0.05). Shaker O et al [12] published data on RBP4 in T2D adult patients, and also found a positive correlation between fatty liver and RBP4 (r=0.7, P=0.001). We also found a positive correlation between ALT and RBP4. Conroy et al [10], also found this relationship in pediatric nondiabetic population. They suggest that RBP4 could be used as an early serum marker of HS, as do we. Our study has some potential limitations. First, its cross-sectional nature does not allow us to establish a causal relationship between RBP4 levels and HS. Second, our small sample size. Nevertheless, to our knowledge, no previous information exists regarding the behavior of in adolescents with T2D and its association to HS.
6. Conclusion
In conclusion, we think that this adipocytokine could be a useful marker of HS not only in obese pediatric patients, but also in pediatric patients with T2D.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
PM, ACHT, LV conceived of the study, participated in its design and coordination. PM, MTV, MK, HM, MM, FH performed the statistical analysis and revised the manuscript critically. All authors were involved in drafting the manuscript. All of them read and approved the final version of the manuscript.