



1. Introduction
In support of the model proposed by Carver and Scheier [1] concerning behavioral self-regulation and personal goal achievement, Scheier, Wrosch, Baum, Cohen, Martire, et al. [2] pursued the concept further by examining how the process of identifying goals that are valued acts as a mechanism by which a person remains behaviorally engaged in life. Valued goals are, in this context, not only objectives, but also reflect the intensity of commitment to attaining these goals, and by inference, the emotions that drive the process of pursuing them. These goals are inherently concrete, meaningful and accessible to consciousness, allowing them to be expressed and evaluated by the individuals themselves. Several tools for strength-based assessment and evaluation have been developed to account for purpose in life such as the Purpose in Life Scale (PIL) [3], the Life Regard Index (LRI) [4], the Life Purpose Questionnaire (LPQ) [5], the Scales of Psychological Well-Being (SPWB) [6], and the Life Attitude Profile Scale (LAP) [7]. According Scheier et al. [2] while these tools are relevant as objective measures of life purpose, valued goals, satisfaction, and psychological well-being, they are often time insensitive (gauging past experience versus current experience), making it difficult to assess changes in purpose in life over time, for example, as a result of pivotal life moments such as illness. These other scales often also measure constructs in addition to purpose in life, such that it is difficult to determine which components within a scale are responsible for producing associations that emerge. It is in this perspective that these authors developed the Life Engagement Test (LET).
The LET is a six-item instrument designed to measure purpose in life by assessing the extent to which people engage in activities they find valuable and significant. This important study describes how psychometric properties of the six items were assessed in eight samples, including four samples of individuals affected by disease [two comprised of cancer patients, one of osteoarthritis patients, and one of spouses of women with osteoarthritis]. Exploratory factor analysis was used to identify a one-factor solution for each of the samples. The LET also showed satisfactory internal consistency for each of the samples (α = 0.72 to 0.87) and temporal stability evaluated over a four-month period in four samples (rs = 0.61 to 0.76). The convergent and divergent validities of the LET were supported by positive and significant correlations with many health-related psychosocial variables, such as self-control and life satisfaction, as well as negative and significant correlations, such as perceived stress and symptoms of anxiety and depression [2]. The authors also found no significant differences between gender, age or ethnic background.
Since its first implementation, much research has documented the direct, positive and significant links between staying engaged in life and several psychological variables, such as psychological well-being [8,9], life satisfaction [10,11], optimism and hope [12], and feelings of personal resilience [13]. In the context of health-related quality of life, life engagement was observed in cases of individuals with prostate cancer to be positively and significantly correlated with a stronger sense of self, feelings of belonging and positive social connections [14], and was shown to reduce perceived (versus real) disabling symptoms associated with Parkinson's disease [15]. The LET has also been shown to be associated with positive changes in health behaviors, such as increased physical activity [9], reduction in smoking [16] and coping with feelings of loneliness [17].
Other works have shown that life engagement mediates relationships between variables such as wisdom and emotional well-being [18], life satisfaction and personality traits, and is involved in a negative correlation with neuroticism [19-21] and a positive correlation with work ethic [19]. Finally, several studies have proposed that life engagement acts as a marker for an adjustment process that promotes successful adaptation [22] and "aging well" [23] through continued volunteering and/or volunteer activities after retirement [24].
There are currently two translated versions of the LET, one in Bangladeshi, the other in Japanese. The Bangladeshi version of the LET [11] was validated with a sample of 210 students in a study on the influence of life satisfaction on life engagement. An exploratory factor analysis identified a one-factor model accounting for 46.80% of the total variance of the Bangladeshi LET. Cronbach's alpha of 0.77 was considered acceptable by the authors. More recently, the Japanese version of LET (LET-J) was validated with two samples of 409 Japanese students (in a test-retest situation) and 439 adult workers [25]. For each sample, exploratory factor analyses confirmed the onefactor structure of LET-J and confirmatory factor analyses revealed good model fits. Cronbach's alphas were also found to be acceptable (α = 0.82 to 0.86). Test-retest reliability for the student sample was also satisfactory (r = 0.76).
To our knowledge, a French translation of the LET does not yet exist. The objective of this study is to examine the reliability and factorial validity of the French version of LET-F from a confirmatory perspective.
2. Method
2.1 Participants
The sample selected allowed for the widest age range. The overall convenience sample consisted of 479 participants, divided into 158 students at the middle and high school levels (83 girls and 74 boys and one blank value; median age 15 years [min. 13 years; max. 17 years]), 138 students enrolled in different disciplines (95 women and 43 men; median age 20 years [min. 18 years; max. 25 years]) and 183 adults (154 women, 29 men; median age 45 years [min. 27 years; max. 72 years]). The first two samples are teenagers and young adults in school or college. The third sample is parents of students.
2.2 Measures
All of them completed the French translation of the LET-F questionnaire, which was developed following a multi-stage procedure [26]. The items in the original version were first translated into French by two of the authors. The resulting French version was then translated back into English by a fully bilingual person who was not familiar with the original scale. A committee composed of two of the authors and an independent bilingual expert who confirmed the quality of the back translation against the source language version and judged their equivalence to be satisfactory. As in the original version, the LET-F includes 6 items, with a positive orientation for three items (items 2, 4 and 6) and a negative orientation for the other three items (items 1, 3 and 5). Each item refers to a statement to which the respondent is asked to indicate their level of agreement on a 5-point scale (ranging from 1 "strongly disagree" to 5 "strongly agree").
For nomological validity, the participants answered the LET-F scales successively and responded to the following questionnaires in their French versions.
Satisfaction with Life Scale (SWLS): this scale measures the cognitive part of life satisfaction. It consists of 5 items evaluated in 7 points ranging from 1 "strongly disagree" to 7 "strongly agree". Cronbach's alpha is excellent (α = .90) [27,28].
Generalized Self-Efficacy Scale (GSE): this scale measures the ability to perform a new or difficult task, or to cope with adversity. This scale involves 10 items evaluated in 4 points ranging from 1 "strongly disagree" to 4 "strongly agree"; Cronbach's alpha is satisfactory to excellent (α = .76 to .90) [29,30].
Perceived Stress Scale (PSS): this scale assesses the importance with which life events are perceived as threatening, unpredictable and painful. It is composed of 10 items assessed in 5 points ranging from 0 "never" to 4 "very often". Cronbach's alpha is satisfactory (α = .78) [31,32].
Hospital Anxiety and Depression Scale (HADS): this tool is divided into two scales which seek to identify an anxious symptomatology for one and a depressive one for the other, as well as the severity of these symptoms. These two scales include 7 items each with 4 points ranging from 0 "very positive valence" to 3 "very negative valence". Cronbach's alpha is satisfactory to excellent for each scale (HADSAnxiety, α = .68 to .93; HADS-Depression α = .67 to .90) [33,34].
All statistical analyses presented below were performed using JASP version 0.12.2. (JASP Team 2020) [35].
3. Results
3.1 Internal consistency, mean, standard deviation, correlations
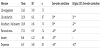
The internal consistency of the French LET-F scale was assessed using the McDonald’s omega (ω) wich is based upon the sum of the squared loadings on the general factor [36]. The French LET-F scale has a satisfactory internal consistency with a McDonald’s omega (ω) of .74, comparable to Cronbach's alpha of the original version between .72 and .80 (see samples 1, 4, 7 and 8 composed of participants with no pathology). These results suggest a certain homogeneity between the items of the scale. The item-total (I-T) correlations show a mean correlation of .66, ranging from .61 (item 6) to .77 (item 3), the average correlation between items is .32. These results are presented in Table 1.

3.2 Confirmatory analysis of the French version of the LET
The factor structure of the scale was verified within the framework of the structural equation models by applying confirmatory factor analysis. Parameter estimates were performed with the Diagonally Weighted Least Squares (DWLS) estimator using the polychoric correlation matrix. This estimator has been evaluated as particularly robust [37] when response scales are ordinal and with skewness and kurtosis showing non-normality of responses (Table 1). The model fit was evaluated on the basis of the following indices and acceptability thresholds: CFI (Comparative Fit Model) ≥ .95, RMSEA (Root Mean Square Error of Approximation) ≤ .06, SRMR (Standardized Root Mean Square Residual) ≤ .08 [38]. Parameter estimates indicate a satisfactory fit to the model in Table 2. Items loadings range from .46 (item 6) to .82 (item 3) and the average variance extracted is 32.9 %.

3.3 LET-F invariance analyses
At the same time, we tested the LET-F for measurement invariance across gender and age variables by performing multigroup confirmatory factor analyses. Due to missing information, invariance analyses for gender were performed on a sample of 478 participants, divided into 332 women (70%) and 146 men (30%) participants. Analysis of measurement invariance for age concerned a sample of 479 participants, divided into two groups: a first group consisted of 296 participants aged 13 to 25 years (M = 17.58; SD = 2.88) and a second group consisted of 183 participants aged 27 to 72 years (M = 45.04; SD = 7.69). For each of these variables, the measurement invariance analysis was tested using four successive nested models: 1/the configural invariance model which poses the invariance of the structure in a single dimension between the groups; 2/the metric invariance model which imposes the equality of the saturations between the groups; 3/the scalar invariance model which adds a constraint of equality of the intercepts for the six items between each group; 4/and finally the strict invariance model which, moreover, forces the identity of the measures of residual variance (measurement errors and specific variance). Successive validation of the first three models is at least a prerequisite for all subsequent comparisons between groups [39]. The results of the analyses of invariance are presented in Table 2. Concerning the gender variable, the results show that the differences in χ2 are not significant between the n-1 model and the n model and that the model fit indices are correct for the models of configural invariance, metric invariance (except RMSEA), scalar invariance and strict invariance, suggesting total invariance for the gender variable.
By contrast, the results pertaining to the age variable reveal significant differences in χ2 and in the adequacy indices between the metric invariance model and the scalar invariance model, too important to consider total invariance for the age variable.
3.3 Nomological validity
This analysis was conducted on a sub-sample of 351 persons (aged 13 to 65 years, M = 50.21, 63.4% of whom were women) of the overall study sample. The size of this sample corresponds to the participants who answered more than 80% of the selected questionnaires. Table 3 presents the correlations between LET-F scores and the other measures (see Measures section: SWLS, GSE, PSS, HADS). The LET-F score is significantly and positively correlated with measures of life satisfaction and self-efficacy, and negatively correlated with perceived stress, depression, and anxiety.
The LET-F scale shows satisfactory correlations close to those obtained in the original study (see samples 1, 4, 7 and 8), with the exception of self-efficacy (proxy measure of self-mastery in our study), which shows lower correlation. On the other hand, the positive associations with life satisfaction and self-efficacy, and negative associations with perceived stress and depression are comparable to those found in the original study.
4. Conclusions
The main objectives of this study were to validate the French version of the LET and to test measurement invariance of LET-F between men and women, and between adolescents/young adults versus adults. The analyses first confirmed the unidimensional structure of the 6-item LET-F, updated in the article by Scheier et al. [2]. The internal consistency of the LET-F was also deemed satisfactory and comparable to those obtained in the samples with no pathologies included in the original English language version. The nomological network of LET-F was also found to be consistent with that found in the original version. Finally, scores observed in the French version shows positive and significant links with well-being variables (life satisfaction and self-efficacy), as well as negative and significant links with adverse variables (perceived stress, and anxiety and depression).
The multigroup confirmatory factor analyses conducted in this study also revealed measurement invariance in the LET-F for gender, confirming that the LET items refer to the same relevant psychological dimension for both women and men respondents. On the other hand, the results revealed differences in response formats according to the age of the respondents, i.e., those under 26 versus those over 26 years of age1. Engagement in life through the pursuit, achievement and evolution of personal goals is not expressed with the same importance, nor with the same judgment criteria according to the two age groups. The absence of age invariance does not point to a weakness in the tool, but rather underlines the way in which each group appropriated the items according to its own frame of reference: "Non-invariance can be informative and may lead researchers to important conclusions about how different groups interpret the same construct" [39]. These data are consistent with lifespan theories that consider that there are necessarily developmental differences in the achievement and design of life goals and objectives according to the life cycle in which the individual is situated [40,41].
1A second analysis was performed without minors (between 18 and 26 vs. over 26 years of age) which did not improve the model: the M3.Scalar model was still rejected.
Taken together, the results of this research thus provide elements of validation for the French version of the LET-F that seem sufficient to envisage its use in the field of psychological research. With its short format (6 items), the LET-F is a brief and relevant measurement scale for assessing respondents' perception of engagement in the lives of the native French speaking population. For Scheier et al. [2] engagement in life is one of the essential components of psychological well-being. Further studies in this field should provide a better understanding of the influence of engagement in life and its varied role in the context of health behaviors surrounding treatment adherence, disease management, coping strategies, behavioral changes, etc., particularly in cases of chronic diseases, from adolescence to old age. These results also lead us to consider the interest and implications of LET-F in therapeutic management. Indeed, it is likely that people who lack purpose in life encounter difficulties in achieving the goals they value because they are too demanding or may have become inaccessible, for example. These perceived difficulties may lead an individual to become less energetically engaged in life, that could lead to discomfort and, potentially, to subsequent manifestations of depression in the most severe cases. This highlights the critical importance for health professionals to identify low levels of purpose in life in their patients and to work with them towards identifying valued life goals, importantly to potentially avoid symptoms associated with depression that could further derail efforts to deal with existing health problems.
In conclusion, the French version of the LET is an instrument with sufficient psychometric qualities to be used in clinical or research settings. For clinicians, the LET-F can be used as a tool to assess a patient's sense of purpose in life based on life events such as illness and bereavement. For researchers, given its brevity, it can be easily combined with other instruments, thus allowing for broad-spectrum investigations of well-being behaviors. However, this study has one main limitation that should guide future research. A time-stability (test-retest) evaluation of the LET-F would provide valuable insight into the stability of the results obtained, which would also allow comparison with the data obtained in the original version [2] and in the Japanese version [25].
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Conception and design: Fabienne Lemétayer and Jean-Baptiste
Lanfranchi
Collection: Manon Florquin and Laura Lepage
Analysis and interpretation of data: Fabienne Lemétayer and Jean-
Baptiste Lanfranchi
Drafting the article: Fabienne Lemétayer and Jean-Baptiste Lanfranchi
Participation in revising the manuscript critically and gave their final
approval of the version submitted: Fabienne Lemétayer, Jean-Baptiste
Lanfranchi, Manon Florquin, Laura Lepage and Laura Saez
Ethics Approvals
Ethical approval has been obtained by the Institutional Review Board (reference number: N° 16-324/ MR 003: 2009422).
Consent to Participate
Informed consent was obtained from all individual participants
included in the study.
Informed consent was obtained from legal guardians.
Written informed consent was obtained from the parents.
Availibility of Data and Material
Data set is available at https://osf.io/xyu4b/?view_only=0021b2bdadd94bc18b8d1641212980be
Acknowledgments
The authors thank Prof. Michael Scheier for his agreement to the translation and validation of the French version of the LET.