



1. Introduction
The global older population has been growing rapidly. Many western countries delivered policies such as “Opportunity Age” in England, “National Strategy for an Ageing Australia”, and “Positive Ageing Strategy” in New Zealand to promote active aging [1]. Recently, some developing countries in Asia such as Japan, Singapore, South Korea and Taiwan have reached the stage where they are aging societies and raised the issue of how an aging population impacts on various areas including productivity [2]. As one of these Asian countries mentioned above, the percentage of Taiwanese older adults above 65 years was over 7% to 10.92% of the total population from 1993 to 2012 and is projected to reach 20% by 2025 [3]. With this increase of the aging population, maintaining and facilitating the well-being of older adults is regarded as integral to achieving active aging in such a society. For sustaining older adults’ well-being in an aging society, the nature and trajectory of change of well-being in older adults need to be investigated.
On the basis of philosophical traditions of what well-being entails, hedonia and eudaimonia, two distinct approaches of well-being, dominate a considerable bulk of research on well-being [4]. The hedonic view on well-being suggested that one can gain the highest level of well-being through maximizing one’s pleasure experience and minimizing one’s affliction, whereas eudaimonic view on well-being contended that actualizing one’s potential and living a virtuous life are key elements and pathways of optimizing one’s personal experience of well-being [5]. Within the hedonic approach, well-being consists of affective and cognitive dimensions. Affective components of hedonic well-being referred to as positive and negative affect and cognitive components of hedonic well-being referred to as life satisfaction [6]. Relative to hedonia, eudaimonic approach stresses positive functioning. Several psychological functioning such as autonomy, self-acceptance, personal growth, life purpose, environmental mastery and positive relatedness were proposed to conceptualize eudaimonic well-being [7,8].
Recently, an integrative view of connecting hedonic and eudaimonic approaches has been proposed to achieve more comprehensive understanding of well-being [9]. The integrative view suggested that pursuits of both hedonic and eudaimonic well-being result in one’s authentic happiness [10]. Peterson, Park and Seligman [11] identified the simultaneous pursuit of pleasure, meaning and engagement, three orientations to authentic happiness, can bring about the highest degree of life satisfaction. For older population, Hyde, Wiggins, Higgs and Blane [12] proposed that control, autonomy, self-realization and pleasure as conceptions of positive functioning in later life, apart from other drivers of quality of life such as health. They also adopted an integrative approach of incorporating hedonic and eudemonic elements to examine older people’s well-being. With a line of integrating two approaches, psychological functioning constituted eudemonic well-being such as autonomy, competence and relatedness may contribute to hedonic well-being. For older people, there are two key conditions (i.e. functional autonomy and perceived emotional support) related to their basic psychological needs and positive functioning mentioned above. Old people with physical or functional impairment may lose their satisfaction of needs for autonomy and competence. Relatedness may provide psychological resources to cope with these impairments and facilitate well-being. In this study, functional autonomy and perceived emotional support these two conditions which older people hold are incorporated to examine their contributions on older people’s hedonic well-being.
Researches on age-related change of hedonic well-being indicate that old people relative to young people increase their well-being as they get older through regulating their emotional experiences and focusing on emotional goals of social interactions [13]. In studies by Ehrlich and Isaacowitz [14] and Scheibe and Carstensen [15], most old people kept a high level of emotional well-being and emotional stability in the final stages of their life, in their 70s and 80s. Gerstorf, Ram, Mayraz, Hidajat, Lindenberger, Wagner and Schupp [16] also indicated that the trend of well-being remains stable but declines dramatically while approaching the end of life using longitudinal data from Germany (The German Socio-Economic Panel Study, SOEP), UK (The British Household Panel Study, BHPS), and America (The U.S. Health and Retirement Study, HRS). In previous studies, larger age ranges (from teenage to nineties) of participants were adopted. Few studies have limited age range for describing change in well-being of the old-old. Hansen and Slagsvold [17] found the Norwegian old people’ well-being decline after about age 70-75 and claimed there are various patterns of age-related change in well-being between young old and old-old age. Consequently, this study focuses on trajectories of well-being of the old-old (above 70 years) using longitudinal data in Taiwan.
As health and functioning decline with age, these life challenges are likely to increasingly cause ill-being. Hsu [18] found an increase in limitations on physical function increases depressive symptoms and reduces life satisfaction in a Taiwanese sample. Smith, Borchelt, Maier and Jopp [19] also suggested that functional impairment limit the German older adults’ well-being especially in their very old age. Similar findings in Hasen and Slagsvold [17], they explained that old people in very old age have less and less coping resources to keep high well-being with their more and more losses in different life domains. This indicates a lack of optimism about the development of older individuals’ well-being. Hence, older individuals’ hedonic well-being is predicted to decline across time accompanying their gradually decreasing physical, cognitive, and social function.
However, the improvement and maintenance of physical function can influence advances in older individuals’ well-being [20]. In addition, a large body of research has documented a significant association between some aspects of social support (i.e. receiving and providing support; instrumental and emotional support) and well-being among the older adults [21-24]. In this study, older individuals who maintain their physical independence and gain emotional support from others in their daily lives are supposed to still experience happiness and satisfaction even in very old age. The benefits of the two factors of functional autonomy and perceived emotional support have been considered separately in past studies, rather than considered together to examine their unique or combined effects. Life course approaches to trajectories of active aging emphasize the connections between individual resources such as physical and psychological adaptation and social resources such as family and peer support. Both in Germany and Great Britain, life satisfaction was found to decrease after the mid 70s until the end of life. The trend was thought to relate to health status and social support [25]. Hence, the contribution of functional autonomy and perceived emotional support to the developmental trajectory of well-being in Taiwanese older adults is examined in this current study.
Social support is a protective factor in functional capacity in the older adults [26,27] and helps older adults to keep their autonomy, which is fundamental for well-being [28]. Newson and Schulz [29] indicated that old people with physical impairment perceive less support and identified the mediation effect of perceived social support in the relation between functional status and quality of life. Landau and Litwin [30] identified the relationship between physical capacity and well-being meditated by psychosocial resources such as locus of control and social network supportiveness among the old-old in Israel. More recently, there has been an emphasis on the combination effects of multiple factors in relation to well-being. The associations between functional autonomy and well-being may depend on which level of social resources i.e. emotional support older adults hold. Therefore, the mediation role of perceived emotional support between functional autonomy and well-being is explored in this study.
The goals of the present study are as follows:
- Describing time-related changes of well-being in old age using multiple measures that cover cognitive and affective dimensions of well-being;
- Testing the differential impact of functional autonomy and perceived emotional support on well-being at each measured time.
- Testing the mediation effect of perceived emotional support on the relationship between functional autonomy and well-being.
2. Method
2.1 Data sources and sample description
Data came from the Taiwan Longitudinal Study on Aging (TLSA) which is nation-representative research, featuring a longitudinal survey which began in 1989. Specifically, the data were taken from three waves of the TLSA conducted in 1999, 2003 and 2007. Detailed information on TLSA data collection is provided by the Health Promotion Administration at the Ministry of Health and Welfare in Taiwan (www.bhp.doh.gov.tw). A total of 2310 participants above 70 years old who completed the survey were incorporated in this study. Educational level of the participants was recorded into no formal education but literate (28.6%), primary school(47.1%), junior high school (9.5%), senior high school (8.7%), college (5.8%), and graduate school (3.3%). The sample mean age in 1999 was 76.38 years (SD=5.2, range 70 to 98 years). 55.3% of the participants were male and 44.7% were female. In 2003, the number of participants reduced to 1743 due to death and incomplete responses (M=79.49; SD=4.55 for age, 53.5% were male and 46.5% were female). In 2007, 1268 participants remained in this study (M=82.82, SD=4.13 for age, 51.0% were male and 49.0% were female). The number of participants increasingly reduced during follow up mainly because people died. Participants’ self-rated health status was recorded into very poor (10.3%), poor (33.2%), common (35.6%), good (15.5%) and excellent (5.5%).
2.2 Measures
Well-being was constituted by the absence of negative affect, and the presence of positive affect and life satisfaction [6]. Owing to the use of secondary data from the TLSA, well-being was operationalized by two available measures of the TLSA: the Center for Epidemiologic Studies Depression Scale (CES-D) and Life satisfaction Rating (LSR). Based on results of prior factor analyses employing database from the TLSA for a 10-item version of the CES-D scale, a scale that is similar to the Iowa version CES-D scale [31], two factors were identified: depressed affect and positive affect [32]. The reliability of the CES-D measured in 1989 is good (Cronbach’s α is .80). Depressed affect could be seen as negative affect. Hence, positive affect and negative affect were measured by the TLSA shorter CES-D scale in this study. Each item was scored from 0 to 3. Positive affect included two items: 1) happiness; and 2) enjoyment of life. Negative affect included eight items such as depression, loneliness, sadness, and fearfulness. These two subscales were summed up separately to produce two total scores (range from 0 to 6 for positive affect scores and range from 0 to 21 for negative affect scores) and then the two total scores were converted into z scores. In addition, the 10-item version of LSR [33] was adopted in the TLSA. Because only four items were measured in 1993, life satisfaction was measured by these four items of the LSR: 1) Compared with others, my life is better than them; 2) These are the best years of my life; 3) I expect I will experience some interesting and pleasant things in the future; and 4) I am satisfied with my life. The reliability of the LSR measured in 1989 is acceptable (Cronbach’s α is .68). Each item was scored 0 or 1. A composite score was formed by summing the four raw scores (range from 0 to 4) and transferring it into a z score.
Functional autonomy can be defined by activities of daily living (ADL) and instrumental activities of daily living (IADL), two components of autonomous life [34]. There were 9 items on individual daily living activities such as eating, dressing and using the toilet and 6 items on instrumental daily living activities such item was scored from 0 to 3. The sum of all scores formed a composite score of functional autonomy (range from 0 to 45) and then was transferred into a z score. A higher score indicated better functional autonomy. The reliability of measures was also good (Cronbach’s α ranged from .95 to .96).
Perceived emotional support in the TLSA was measured by the degree to which: 1) Family/relatives/friends care about you; 2) Family/ relatives/friends listen to you; 3) You could count on someone from family/relatives/friends when you were ill; and 4) You were satisfied with the care and support you received from family/relatives/friends. Each item was scored from 1 to 5. The sum of all scores formed a composite score (rang from 4 to 20) and then was transferred into a z score to create a continuous metric. Higher scores indicated perceiving more emotional support from others. The reliability was .97, .98 and .99 in 1999, 2003 and 2007, respectively.
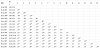
The correlation matrix among these variables i.e. positive affect, negative affect, life satisfaction, functional autonomy, and emotional support can be seen as Table 1.
2.3 Data analyses
Most previous studies used the hierarchical linear model (HLM) to deal with longitudinal raw data but the HLM couldn’t consider measurement models incorporating latent variables, temporal measurement invariance and residual dependence across time. The multiple-indicator multilevel (MIML) growth model was proposed to incorporate measurement models as a foundation of whole model [35]. Because the same measures were used across three time points in present study, the residuals of the same subscales were specified to be correlated in the MIML growth models. Mplus version 5.21 [36] was used to generate fit indices and parameters of all MIML growth models. All observed variables were checked the assumption of normality with the Kolmogorov-Smirnov test before conducting MIML growth models. Results showed that all these variables are not normally distributed. MLR which are robust to non-normality and non-independence of observations would be used to an estimator for MIML models [36]. The overall fit indices of well-being trajectory models were assessed using the Comparative Fit Index (CFI), Tucker- Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR). The criteria of fit indices were used as follows: CFI>.95, TLI>.95, RMSEA <.06 and SRMR <.08 [37].
3. Results
The MIML growth model had good model fit (CFI=.99, TLI=.99, RMSEA=.02, and SRMR=.02, see Table 2). The scaling constant and unit of the latent variable were identified to remain the same for the observed indicators across all three time points through testing equality of the indicator intercepts and factor loadings. The mean of the slope growth factor was estimated to be-.321, indicating a decreasing trend during 9-year period.A significant negative relationship between intercept and slope (r=-.290, p<.001) indicates that the higher the initial well-being, the less it decreased over the 9-year period ( Figure 1).

Furthermore, age and gender were incorporated into the model 2. As seen in Table 2, the model with two time-constant predictors also had good model fit (CFI=.97, TLI=.97, RMSEA=.03, and SRMR=.03). The influence of age on well-being only appeared at the baseline (β=- .106, p<.01). Old-old adults had less well-being relative to young-old adults. There were significant gender effects on both intercept and slope factors of the latent growth model (β=.187, p<.001 and β=-.123, p<.05). In an initial stage, old men had more well-being compared with old women. With time passing, old men’s well-being decreased less sharply than old women.
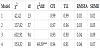
The above model was extended to incorporate perceived emotional support and functional autonomy, two time-varying covariates(model 3). The results indicated an acceptable model fit for the model (CFI=.93, TLI=.90, RMSEA=.04, and SRMR=.09, see Table 2). Both emotional support and functional autonomy were demonstrated to contribute to older adults' well-being at each wave (βw1=.44, p<.001, βw2=.42, p<.001; βw3=.36, p<.001; and βw1=.63, p<.001; βw2=.62, p<.001; βw3=.62, p<.001 for perceived emotional support and functional autonomy, respectively). And all the β weights described above indicated that functional autonomy is relatively more important to well-being than perceived emotional support across all three time point.
After adding perceived emotional support and functional autonomy into the model, age and gender effects on the level and change of well-being were no longer significant. The older old adults had less functional autonomy relative to younger old adults at each wave (βw1=-.41, p<.001, βw2=-.44, p<.001, βw3=-.43, p<.001). There were no significant differences of age on perceived emotional support. Compared with women, Taiwanese old men had better functional autonomy (βw1=.20, p<.001, βw2=.21, p<.001, βw3=.18, p<.001). Inverse effects of gender on perceived emotional support were found at wave 2 and 3. That is, women reported more perceived emotional support than men while getting older (βw2=-.06, p<.001, βw3=-.07, p<.001).
The mediation effects of perceived emotional support on relationships between functional autonomy and well-being were added into the model 4 (Figure 2). In comparison to the previous model, this model yielded that there was a slight improvement on indices of model fit (χ2 diff (6) = 49.59, p<.001, CFI=.94, TLI=.91, RMSEA=.04, and SRMR= .07, see Table 2). Both Perceived emotional support and functional autonomy were found to have significant positive direct effects on well-being (βw1=.43, p<.001, βw2=.41, p<.001; βw3=.35, p<.001; and βw1=.61, p<.001; βw2=.60, p<.001; βw3=.60, p<.001 for perceived emotional support and functional autonomy, respectively). There were some indirect effects of functional autonomy on well-being through its impact on perceived emotional support (β=.12, p<.001 for functional autonomy to perceived emotional support at wave 1; β=.07, p<.001 for functional autonomy to perceived emotional support at wave 2). There was a small mediating effect of perceived emotional support on relationships between functional autonomy and well-being.

There were similar findings on age and gender effects from model 3 and model 4. There were still no significant age and gender effects on the level and change of well-being. Old-old adults had less functional autonomy than young-old adults (βw1=-.41, p<.001, βw2=-.44, p<.001, βw3=-.42, p<.001) and female old people had less functional autonomy than male old people (βw1=.18, p<.001, βw2=.22, p<.001, βw3=.20, p<.001) at each wave. Female old people also perceived more emotional support than male when they became older (βw2=-.06, p<.001, βw3=-.07, p<.001).
4. Discussion and Conclusion
The pattern of well-being upon a restricted age range in Taiwanese older adults sample was identified. A trend of declining well-being over a 9-year period was found in Taiwanese older adults aged 70 and above. The negative relationship between the initial status and the growth rate of well-being in this study indicated that the higher the individual’s initial state of well-being, the slower the individual’s decrease in rate of well-being. The result implied that the psychological capital people held and accumulated in the initial time is a core predictor for their future well-being.
With a decreasing trend of older individuals' well-being in Taiwan, the trajectory of well-being of Taiwanese older adults was confirmed to be promoted by their perceived emotional support and functional autonomy. This result is similar to previous findings [22]. Comparing the relative influence of perceived emotional support and functional autonomy on well-being, functional autonomy was found to be more essential than perceived emotional support. Gabriel and Bowling [38] adopted in-depth interviews to gain older individuals’ perspectives on the quality of life and also found retaining independence and avoiding dependency on others are important for their late-life qualities. The result of this study indicated that keeping independence is still a core need for old people.
Age and gender were incorporated into the MIML growth models to account for between-person variation in trajectories of well-being. The result indicated that old people with older age had lower wellbeing at the initial stage. Age difference did not have an influence on the change rate of well-being across time. Compared with females, male old people had higher well-being at the initial stage and a slower rate of decrease in well-being across time. As a result of genderstereotypic socialization, women are encouraged to express their emotions and men are taught to inhibit their emotions to avoid being feminine [39-41]. In addition, a similar finding was presented in Carmel and Bernstein [42]. They found that the decline of wellbeing with age can be mainly attributed to losses of control in life for old men but not for old women. In this study, older male participants were survivors. They had better functional autonomy and control in life, hence expressed higher well-being.
While adding functional autonomy and perceived emotional support, there were no age and gender differences on the level and change of well-being. The result showed that younger old people had better functional autonomy than older old people and men had better functional autonomy than women over time. Age and gender differences in trajectories of well-being are mainly mediated by functional autonomy across time. Elder women experienced more health-related problems and functional disabilities than men. The feeling of functional disabilities causes elder women perceived less psychological well-being. As a result, as predicted by a classical model of well-being, older individuals’ decreasing well-being across time could be attributed to their losses in health and relatives with aging [25,43].
Perceived emotional support was also demonstrated to enhance older individuals’ well-being across time. There were no mediation effects of perceived emotional support on association between age and well-being. This implied that most old people have stable social networks and have similar feelings of emotional support from significant others no matter which age group they belong to. Darbonne, Uchino and Ong [44] also did not find the mediation effect of social support on association between age and well-being and suggested considering the negative dimension of social relationships. Gender difference on well-being was mediated by perceived emotional support. Old women experienced more emotional support than men. The emotional support perceptions between different gender groups further influence older individuals’ well-being.
The combination effects of perceived emotional and functional support on well-being were positive. By putting the mechanism of perceived emotional support and functional support together, small indirect effects of functional autonomy on well-being mediated by perceived emotional support were found. The result is consistent with previous studies [29,30]. In an interdependent culture, older adults may avoid seeking help to save face and keep social harmony despite their personal needs [45]. Receiving support from others may inhibit an individual’s sense of autonomy and reduce selfesteem. Hombrados-Mendieta, Garcı´a-Martı´n and Go´mez- Jacinto [46] investigated how different types of social loneliness (i.e. family, romantic, social loneliness) mediated different types of social support (i.e. emotional, informational, and instrumental support) and different sources of such support (i.e. family, partner, friend, and community) on well-being in a Spanish sample. They found there were complex patterns among these variables. Further studies could conduct multidimensional analyses to explore the influence on well-being of different kinds of social support and different sources of supports under an interdependent culture. Hence, the mechanism among social support, functional autonomy, and well-being could be explored more precisely.
Several limitations in this study highlight areas for future research. First, findings are restricted to responses from survivors cover all three waves in TLSA. Limited information on changes of well-being across time was gained from these survivors with better functional status and social network supportiveness. With a representative sample of older adults including the persons who dropped out due to other reasons, age patterns in well-being and contributions of functional autonomy and social support may have been different. Second, only self-report data used in this study may not reflect true differences in objective conditions.
The unique contribution of this study was to integrate functional autonomy and perceived emotional support into models for explaining well-being trajectories. Decline of functional autonomy with ageing indeed reduced older individuals’ well-being across time, but emotional support can protect older individuals to keep their well-being.
Competing Interests
The author declare that there is no competing interests regarding the publication of this article.
Acknowledgments
The author would like to thanks the Population and Health Research Center, Bureau of Health Promotion, Department of Health, Taiwan, Republic of China, for providing the data.