



1. Introduction
In Portugal, 13% of the population suffer from Type 2 diabetes [1]. Diabetes is known to cause multiple medical, psychological and sexual problems in both men and women [2,3]. According to Schover [4] and Wandell and Brorsson [5], dyadic relationships may suffer changes after a diagnosis of a chronic disease and, as a result, sexual difficulties may arise in the couple. In fact, marital support is an important aspect when the couple has to deal with a chronic disease [6,7]. The influence of dyadic adjustment is greater when one of the elements has to deal with the complexity of the diabetes regimen (e.g. buying and preparing food, medication administration, getting involved in physical exercise) [6]. Literature shows that couples presenting less marital satisfaction [8-11], report less communication and problem resolution skills [12,13] and more difficulty in handling tasks related to diabetes. Patients’ self-care behaviors decrease when there is conflict in the relationship and criticism has been associated with a poor glycemic control [14]. However, several studies have shown that patients with diabetes report a good marital adjustment, higher satisfaction with disease management (treatment, appearance, activity), a lesser impact of diabetes on their lives as well as less emotional stress related to diabetes [8-11,15]. In fact, Trief and collaborators [8] reported that better dyadic adjustment was associated with a better adaptation to diabetes, less emotional distress, and better quality of life. The authors also found that the marital relationship was a better predictor of glycemic control than family support. A supportive partner was associated with the patient’s quality of life, adjustment to the illness [16], and adherence to self-care behaviors [17].
Sexual problems may be a consequence of diabetes and may lead to a lack of adherence to treatment and problems in intimate relationships [18]. Sexual problems that are not recognized may impair quality of life [18] and the quality of the intimate relationship. In fact, several studies reveal that better dyadic adjustment has been associated with better sexual functioning [19-23] and marital satisfaction had a positive impact on sexual satisfaction [23]. Women with diabetes, with high prevalence of sexual dysfunction also showed lower satisfaction with the marital relation, lower quality of life and more depressive symptoms [24-26]. Recently, Pedersen et al. [27] found that sexual desire and low satisfaction are often reported among men and women with diabetes. Therefore, sexual satisfaction needs to be taken in consideration given its fundamental role on sexual health and wellbeing [28].
According to the literature, sexual dysfunctional beliefs are associated with less sexual satisfaction [29]. Sexual education decreases be-liefs in sexual myths [30] since many beliefs held about sexual attitudes and behaviors are based on stereotyped views of sexuality. Not having accurate sexual information has been related to less sexual satisfaction. In a study that addressed beliefs regarding what is “adequate”, “ desirable” and “too short” or “too long” intravaginal ejaculatory latency time among those with sexual dysfunction, dysfunctional beliefs were correlated with impotence, premature ejaculation and dissatisfaction. Therefore, sexual beliefs may affect the patient’s quality of life and lead to distress and displeasure. Since stereotype is the main determinant of expectation, dissatisfaction due to wrong perception, may impact significantly the individual’s self-esteem and quality of life causing emotional distress and leading to relationship problems [31]. Sexual health in diabetes is a very important topic and has been defined as the integration of somatic, emotional, intellectual and social aspects in ways that are positively enriching [32] with an impact on how the individual perceives and manages one’s sexuality, setting a norm against which people identify “sexual problems”. However, few patients openly discuss sexual problems with their family physician [18]. At our knowledge, there are only one study about the role of sexual dysfunctional beliefs and sexual satisfaction in women and men with diabetes, that showed that women with diabetic husbands showed a higher mean score in sexual dysfunctional beliefs than women with non diabetic husbands [33].
One of the consequences of diabetes includes sexual dysfunctions and sexual dissatisfaction. Sexual disorders among men with diabetes may affect quality of life significantly because there is a high likelihood of developing vascular and neurological complications that result from hyperglycemia as well as psychological problems [34] or a combined effect of some of these factors [35-37]. As a result, some patients are reluctant to take their medication lowering their adherence to the diabetic regimen. Adherence to self-care behaviors is an important issue for clinicians. Non-adherence is considered a public health problem [38]. The low rate of adherence may adversely affect disease progression and consequently, quality of life [39] resulting in an increase in mortality, number of consultations, hospitalization and/or unnecessary costs to the health care system [40,41]. Non-adherence to medication is a major issue in diabetes since adherence is essential in the prevention of diabetes complications [42].
According to a recent systematic review about sexual satisfaction [28], there are many factors that contribute to sexual satisfaction, such as: individual factors (socio-demographic and psychological variables), factors related to intimate relationships and sexual response; factors re-lated to social support and family relationships and finally, factors related to cultural beliefs and values. In this study, the focus was in individual factors (sociodemographic and clinical variables as well as sexual dysfunctional beliefs and sexual information) and intimate relationships (dyadic adjustment), in order to explore their contribution to sexual satisfaction, in patients and partners.
In Portugal, very few studies have addressed the impact of the predictors of sexual satisfaction in patients with diabetes and their partners. Therefore, this study focused on: 1) differences on psychological variables according to gender, education level, age and duration of illness; 2) the relationships among dyadic adjustment, sexual information, dysfunctional sexual beliefs, adherence and sexual satisfaction; 3) predictors of sexual satisfaction in patients and partners.
2. Methods
2.1 Sample
Participants were 87 patients with type 2 diabetes and their partners (n= 174). Average age was 62 years old for male patients (SD: 12.52) and 59 years old for female patients (SD: 14.1). In this sample, 49% of patients completed elementary school, 18.3% finished high school and 8.7% has a university degree. Diabetes duration was 12 years on average (SD: 9) for male patients and 9 years (SD: 7.0) for female patients. Regarding the marital status, 93% of patients were married. 47% of male patients and 77% of female patients showed diagnosed diabetes complications such as retinopathy and nephropathy. Only 6% of males and 3% of females reported having difficulty with sexual performance. Age average for male partners was 50.65 years old (SD=2.45) and 61.67 years old for female partners (SD=2.09). In terms of education, 4.8% of partners finished ele-mentary school, 20.3% high school and 6.3% a university degree.
Patient’s recruitment was conducted in two institutions in the North of Portugal: an Association of Patients with Diabetes and a Central Hospital where patients received their routine diabetes care. The procedures involved a first telephone contact introducing the study and inviting patients to participate with their partner. When the patient agreed to participate, an appointment before or after the next routine consultation was set. The couple signed a written consent before answering the questionnaires. Exclusion criteria for participation were: 1) having a psychiatric disorder and 2) having other chronic disorder or medical condition affecting sexual functioning (e.g. paraplegias). Patients from the Association were no different than those from the hospital, in clinical and socialdemographic characteristics.
2.2 Instruments
In order to study individual and couple's variables in patients with diabetes and their partners, the following instruments were used:
- Dyadic Adjustment was assessed by the Revised Dyadic Adjustment Scale (RDAS) [43,44] a 14-item questionnaire composed of three subscales: cohesion, satisfaction and consensus. Items are presented in a 5-point-scale. A higher score indicates better adjustment. In this study, only the total scale was used. Reliability in this sample was .76.
- Dysfunctional Beliefs were assessed with the Sexual Dysfunctional Beliefs Questionnaire (SDBQ) [45]. This questionnaire has a femi-nine and a masculine version. It is composed of 60 items that assess specific sexual beliefs, considered relevant in the development of sexual dysfunctions, in 6 subscales: beliefs regarding sexual conservatism, sexual desire as sin, aging, body image, affection and maternity. The male version has the following domains: sexual conservatism, female sexual power, ‘macho’ beliefs", beliefs about women’s sexual satisfaction and restricted attitude toward sexual activity. Items are presented in a 5-point-scale. In this study, only the total scale was used. A higher score indicates more dysfunctional beliefs. Reliability in this sample was .91.
- Sexual Beliefs and Information were assessed with the Sexual Beliefs and Information Questionnaire (SBIQ) [46,47], a 20-item questionnaire that assesses information and sexual knowledge in 5 subscales: availability, stress/pressure, aging, sexual satisfaction and basic information. In this study, only the total scale was used. Items are presented in a 5-pointscale. A higher score indicates more correct sexual beliefs and information. Reliability in this sample was .70.
- Sexual satisfaction was assessed with the Index of Sexual Satisfaction (ISS) [47,48], a 25 item questionnaire that assessed degree, severity or magnitude of a problem with the sexual component of a couple’s relationship. Items are presented in a 5-point-scale. A higher score indicates more sexual problems. Reliability in this sample was .90.
- Adherence was assessed with the Diabetes Adherence [49], a 5-item questionnaire that assesses adherence to self-care behaviors, in patients, regarding diet, physical exercise and medication. Items are presented in a 5-point-scale. A high score indicates lower adherence. Reliability in this sample was .75.
2.3 Data analysis
In order to examine differences according to gender a t test was performed as well as chi square tests regarding education, age and illness dura-tion, on all psychological variables. A Pearson correlation was done to analyze the relationships among patients and partners variables. To test the differences between patients, according to gender, education level, age and illness duration, a Kruskal-Wallis test was performed. Predictors of sexual satisfaction were tested using a multiple regression analysis (method enter) for patients and partners. In the first block, gender and illness duration were introduced and in the second block, the psychological variables (dyadic adjustment, sexual dysfunctional beliefs, and sexual beliefs, and information).
3. Results
3.1 Differences on patient’s Psychological Variables according to Gender, Education Level, Age and Illness Duration
Differences were found on dyadic adjustment, sexual satisfaction and sexual dysfunctional beliefs. Female patients presented more marital adjustment (t=2.23, p≤.05) and sexual dysfunctional beliefs (t= 4.86, p ≤.001) than male patients. On the other hand, male patients showed more sexual satisfaction than females (t= 2.66, p≤.05).
Patients with elementary school education had more dysfunctional beliefs than those with a college education (χ2=19.5, p ≤ .000) and the latter had more correct sexual information (χ2 =8.90, p≤ .012). Younger patients (< below 65 years old) showed more adherence (χ2 =22.3, p ≤ .000) and the oldest group ( ≥ 65 years old) presented more dysfunctional beliefs (χ2 =63.8, p ≤ .000) when compared with the younger and the middle age groups (between 51 and 64 years old). Older women reported better sexual functioning than younger women (χ2 =8.07, p ≤ .018). Regarding illness duration, patients with diabetes less than 10 years presented more dysfunctional beliefs than those between 10 and 24 years or longer than 25 years (χ2 =6.76, p ≤ .034).
3.2 Relationships between Dyadic Adjustment, Sexual Information, Dysfunctional Sexual Beliefs, Sexual Satisfaction and Patients’ Adherence
The results revealed that adherence was positively related with sexual information (r=.254, p≤.05) and negatively with dysfunctional beliefs (r=-.310, p ≤.00), in patients. No partner’s variables correlated with patient’s adherence.
3.3 Relationships between Dyadic Adjustment, Sexual Information, Dysfunctional Sexual Beliefs and Patient’s Sexual Satisfaction
Sexual satisfaction was positively related to dyadic adjustment (r=5. 30, p ≤. 001) and negatively with dysfunctional sexual beliefs, in patients (r=-. 215; p≤. 05.) Patient’s sexual satisfaction was also positively related with partner’s sexual information (r= .269; p≤.05), dyadicad
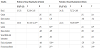
3.4 Predictors of Sexual Satisfaction in Patients and partners
In patients, the model of the regression analysis showed that gender and sexual dysfunctional beliefs were positive predictors of sexual dissatisfaction and dyadic adjustment was a negative predictor, in patients, explaining 38% of the variance.
In partners, the model of the regression analysis showed that gender and sexual dysfunctional beliefs were positive predictors of sexual dissatisfaction and dyadic adjustment was a negative predictor, in partners, explaining 22% of the variance (Table 1).
4. Discussion
One goal of this study was to find differences according to gender, education, age and illness duration, on all psychological variables. Results showed that female patients presented higher marital adjustment and sexual dysfunctional beliefs than male patients. Nobre and Pinto- Gouveia [50] found females to have more dysfunctional beliefs than males particularly regarding age and body image. Also, according to Adams and collaborators [46], more incorrect sexual information was associated with sexual dysfunctional beliefs. In fact, sexual dysfunctional beliefs are considered a moderate risk factor for sexual problems [50]. On the other hand, male patients showed more sexual satisfaction than females. Verbrugge [51] and Kandrack, Grant and Segall [52] found similar results and less burden in males regarding diabetes when compared with females [53].
Patients with elementary school education had more dysfunctional beliefs than those with college and the latter had more correct sexual information. In fact, more education may provide access to better and more resources as well as information regarding diabetes [54,55].
Younger patients showed more adherence. This result is intuitive since younger patients may be more concerned with the possible complications of diabetes and their impact on sexual performance. Older patients reported more dysfunctional beliefs, which is in accordance with other studies [5,56]. Also, older women reported better sexual functioning than younger women. Studies are controversial regarding the impact of age on sexual satisfaction since some studies found a positive effect [23] and others a negative impact [57]. In this case, differences were found on sexual functioning with women reporting better sexual functioning. One may hypothesize that older women may be less demanding regarding their sexuality performance than younger women. This hypothesis needs to be pursued further.
In terms of illness duration, those with diabetes for less than 10 years presented more dysfunctional beliefs than those with a longer illness duration. Patients who have been living with the illness for a longer period of time may have learned more accurate sexual information and, as a result were able to correct their sexual beliefs. This hypothesis also needs to be pursued between in future studies. Another goal of the study was to explore the relationship between the psychological variables, in patients and partners. Results revealed that adherence was positively correlated with sexual information and negatively with dysfunctional beliefs, in patients. This result emphasizes the importance of providing accurate information on sexuality to diabetes patients in order to increase adherence to selfcare behaviors and decrease sexual dysfunctional beliefs [39,40,42]. Patients with more information regarding sexuality may be more motivated to follow the diabetic regimen and, therefore, adhere to self-care behaviors since they become aware of the consequences of non-adherence, on their sexual performance. Future studies should address this issue further. However, no partner’s variables were correlated with patient’s adherence. This result is interesting since partners’s dyadic adjustment was found to predict patient’s adherence to self-care behaviors in recent diagnosed patients (less than a year) [58]. One may hypothesize that, in this case, since average for diabetes diagnosis was 12 years, partners’ dyadic adjustment and sexual beliefs may become a more prominent issue when the couple is struggling with the adaptation to diabetes, right after the diagnosis. Future longitudinal studies should test this hypothesis.
Also, sexual satisfaction in patients was positively related to dyadic adjustment, emphasizing the fact that the quality of marital adjustment is associated with more sexual satisfaction, as the literature have shown [19-23]. However, sexual satisfaction was also negatively related to dysfunctional sexual beliefs, indicating that sexual beliefs play an important role in sexual satisfaction [18,29-31]. Therefore, it is important that patients receive correct information about sexuality to change erroneous beliefs, in order to increase sexual satisfaction. These results are in accordance with Adams and collaborators [46], who found beliefs and incorrect sexual information to be related to sexual problems. In fact, problems in sexual functioning may have a negative impact on a couple who is already trying to adapt to a chronic illness such as diabetes.
Patient’s sexual satisfaction was also positively related with partner’s dyadic adjustment, partner’s sexual information, partner’s sexual satisfaction and negatively related with partner’s dysfunctional beliefs. These relationships were expected since variables related to intimate relationships have been associated with sexual response [21,28].
Finally, female gender, having more sexual dysfunctional beliefs and a reduced dyadic adjustment were predictors of sexual dissatisfaction in patients and partners. Female’s patients and partners report more burden associated with diabetes when compared with males [51-53], and this is also true in the case of sexual satisfaction, in this study. Sexual dysfunctional beliefs play an important role in sexual satisfaction [18,29-31], in both patients and partners, which may be related, in this study, to the sample’s age. In fact, in this sample, the mean age of patients, was 62 and 50 years for patients and partners, respectively. At this age, it is possible that couples base their beliefs on moral criteria, centered on reproduction, and the prevalent sociocultural norms and values, reporting, as a result, more dysfunctional beliefs that may relate to sexual dissatisfaction. A negative dyadic adjustment affects sexual functioning what may explains its predictive role regarding sexual dissatisfaction [21].
The results of the present study emphasize the need for sexual satisfaction and sexuality, in general, to be addressed in medical and nursing routine clinic visits in patients with diabetes. Sexual information and dysfunctional beliefs are particularly relevant for the patient’s adherence.
This study shows the importance of including the partner in the “sexuality conversations” when addressing diabetes management, with the patient. Other studies have shown the important role of the partner in the promotion of adherence to medication and selfcare behaviors, in pa-tients with diabetes type 2 [17,59,60]. Finally regarding sexual health, this study highlights the intrinsic relationship between sexual beliefs, dyadic adjustment and adherence, in patients with diabetes type 2 and their partners, emphasizing the need to use a dyadic approach.
5. Limitations
Due to the sample size in this study, generalization of results is limited and interpretation should be cautious. The sample was also collected in a very conservative Catholic region regarding sexual beliefs and reported a low level of sexual dysfunctions. Future studies should include bigger samples, include non-Catholic patients and take into consideration marriage duration.
6. Conclusion
These results suggest the need for psychological intervention in patients and partners, regarding sexual dysfunctional beliefs and dyadic adjustment taking into consideration their importance for sexual satisfaction. Patients often do not communicate with physicians or partners, as openly and as often as needed, to optimize sexual functioning. Therefore, physicians should include partners when addressing the impact of diabetes on the couple’s sexual satisfaction and an open discussion of sexual problems should be a standard procedure in diabetes routine clinic visits.
Competing Interests
The authors declare that they have no competing interests.