


1. Introduction
Patients admitted to the Intensive care unit (ICU) are seriously ill and often suffer from chronic critical illnesses. These patients receive multiple medications from a variety of pharmacological classes due to life threatening illnesses. They are a unique group of population with diverse disease processes, existing or impending multi organ failure and potentially altered pharmacokinetic and pharmacodynamics characteristics onto which pharmacotherapy is added [1]. Drug therapy in critically ill is therefore complicated. The judicious use of these medications can be lifesaving. The routine use of conventional drug dosage regimens may expose a substantial portion of ICU patients to drug related problems such as treatment failure, drug interactions and high risk of adverse drug reactions. Careful titration of dosage regimens becomes imperative to ensure the ideal treatment outcome [2]. Antimicrobial agents are one of the frequently utilized drug classes in an ICU setting. Patients with critical illnesses are at higher risk of developing nosocomial infections and antibiotics are the most powerful and useful tools to manage these infections.
Extensive and indiscriminate use of antimicrobial agents has been documented in ICUs in previous published reports. [3,4]. The widespread use of broad-spectrum antibiotics has led to the emergence of several resistant strains of microbes. These contribute significantly towards rise in the escalating health care costs and patient morbidity and mortality [3,4]. Therefore, monitoring and evaluation of prescribing patterns of antimicrobial agents are one of the recommended strategies to contain and control resistance also to improve the prescribing practices. Drug utilization study is a component of medical audit that does monitoring and evaluation of the drug prescribing patterns and suggests necessary modifications in prescribing practices to achieve rational therapeutic practice as well as cost effective health care [5].
The inappropriate and unnecessary use of antibiotics is a common practice in health care setting [6,7]. It has been observed that irrational utilization of antibiotics lead to an escalation in the morbidity and mortality rate in community, healthcare cost and development of resistance against antibiotics [8,9]. Appropriate use of antibiotics could be promoted by use of an antibiotic stewardship program like drug utilization evaluation (DUE) with an aim of maximizing the therapeutic response while limiting the unintended side effects [10]. DUE is ongoing, systematic criteria- based evaluation of drug use that helps to ensure that medicines are used appropriately at an individual patient level [11]. The overall objective of DUE is to promote rational medication use. Antibiotics are one of the most common drugs prescribed in hospitals today. The use of antibiotic in hospitals has been a major concern in the last few decades for several reasons. It has been estimated that up to two third of all patients receive at least one antibiotic during hospitalization and the cost involved is therefore correspondingly high and up to 40% of a total hospital‘s drug expenditure may be devoted to the purchase of antibiotics [12]. From Administration point of view, it has contributed to the significant rise in hospital budget. Furthermore, from community perspective, inappropriate usage of antibiotic is considered a major reason for development of drug resistance against various pathogens. Similarly, patients have also suffered in the past due to increased side effects of antibiotics [13].
Meropenem is a broad spectrum restricted antibiotic effective against Gram positive and Gram-negative organism and also against anaerobes. Various researchers have proved that meropenem is equally or more effective than conventional choices in conditions like febrile neutropenia and urinary tract infections, thereby increasing the frequency of prescriptions [14,15]. The objective of this study was to evaluate the meropenem utilization among patients in the ICU in military hospital, Khartoum Sudan.
2. Materials and Methods
Study design: A longitudinal observational retrospective study was carried out during the period from September 2014 to February 2015.
Study area and study population: All files of patients attending intensive care unit(ICU)in military hospital, Khartoum, Sudan during the study time and using meropenem as antibiotics were included.
Study instrument: A well-designed format was used to collect the data. The total sample size of 135 files was gathered. The data collected included two parts. The first part composed from questions about patient' age, weight, gender and any medications used other than meropenem. The second part constituted from questions about meropenem uses; dose, duration of uses, therapeutic outcome, and type of infection, results of bacterial culture test and creatinine clearance of patients (Table 1).
Study was approved by the committee of postgraduate studies, Faculty of Pharmacy, Omdurman University, and permission to access the data in the patient records anonymously was obtained from the Military Hospital administration.
Data analysis: The collected data was processed using Statistical Package for Social Sciences (SPSS) windows software version 17. Mean, frequencies as percentages were used to describe variables (Table 2).
3. Results
A total 135 patients files who’s used meropenem during hospitalization were analyzed. More than half 73 (54.0%) of them were female. The majority 74 (54.81%) of investigated patients were older than 60 years, Table1. Meropenem was prescribed for all patients without culture documented therapy or as prophylactic therapy. The majority of meropenem indications were as empirically 108 (80%), followed by septicemia 17 (12.59%), and pneumonia 10 (7.41%) Figure 1.
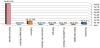
Slightly more than half 70 (51.85%) of meropenem prescribed was in combination with other antibiotics. The dominant combined antibiotics were ceftriaxone 1000 mg 51 (72.86%), followed by ciprofloxacin 200 mg 13 (18.57%), Figure 2.

Table 2 shows the dosage of meropenem used; 0.5-1 gm each 12 hours was the most common dosage used 1 (60%), while 0.25-0.5 gm twelve hourly was the least common dose 7 (5.19%). The dominant duration days were 5-10 days 81 (60%).
One fifth of patients received meropenem were died, while 88 (65.2%) of them were well controlled after using this atibiotic, Figure 3.

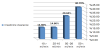
Figure 4 shows the creatinine clearance among the patients received meropenem. A total 55 (40.7%)of patients were normal creatinine clearance level, so they didn’t need dose adjustment, while 40 (29.6%) out of the patients had mild renal failure with creatinine clearance level between 26- 50 ml/min so they need dose adjustment, and 20 (14.8%)of them suffered from severe renal failure, since their creatinine clearance level was less than 10 ml/ min.
4. Discussion
Meropenem is an antibiotic that is often used for empirical treatment of infections in critically ill patients with acute kidney injury. It has clinically insignificant protein binding (2 to 3%) [16].
Proper educational, financial and regulatory programs directed towards health care professionals must be organized to promote rational use of meropenem. In addition provision of standard treatment guidelines, accompanied with onsite training and supervision may be helpful in guiding physicians in the appropriate use of meropenem in particular and antimicrobial in general.
Meropenem use evaluation in this study appears to be inconsistent with evidence based assessment criteria. The most evident inappropriateness was observed when meropenem was used as an empirical therapy. Physicians were used this antibiotic empirically for patients admitted to the ICU without determination the exact infection. They might think that all patients admitted to ICU are in a critical situation and with a high suspected infection. The study also detected other potential problematic areas where concordance with standard guidelines is yet to be achieved. The direct correlation between occurrence of side effects and declining renal function suggests the use of therapeutic drug monitoring in routine practice especially in renal compromised patients. Continuous medical education, functional drug and therapeutic committees and regular drug utilization evaluation programs could help in accomplishing the milestone of rational medication use. Efforts of individuals may not change the practice altogether, but it could influence on the numerous negative aspects of antibiotic usage in healthcare practice.
The clinical setting in the medical ICU warrants the use of drugs from various drug classes [17]. Rational prescription of drugs is essential for better patient care. The firststep in any intervention programme to improve drug utilization is to assess the extent of existing problem in prescribing [18]. As far as we know this is the first study was conducted in Sudan to evaluate drug utilization meropenem in ICU patients in military hospital.
The results of this study revealed that the majority of patients received meropenem were above 60 years old. Also 29.6% of them suffered from moderate to severe renal failure. This is probably for an excellent safety profile of meropenem in elderly and renally impaired patients which reported by Cunha 1998 [19].
In the current study overall meropenem was prescribed without culture; which means that the drug was used depending on prescribers' experience or on the basis of clinical decision, but not on culture based. This was in agree with a study conducted to evaluate the use of carbapenem in a French University hospital by Jary et al., which found60% of meropenem was prescribed empirically [20].
The high therapeutic outcomes reported in this study was constant with a results reported by Cohen et al., which found that the majority of patients treated with meropenem met the therapeutic success [21].
In this study vancomycin was combined with meropenem in 8.57% of prescriptions, which conform with a suggestion by Stan, 2009 that; a combination of a β-lactam antibiotic with vancomycin may provide benefits in a therapy for serious MRSA infection [22].
5. Conclusion
Meropenem use evaluation in this study appears to be inconsistent with evidence based assessment criteria. The most evident inappropriateness was observed when meropenem was used as an empirical therapy. The study also detected other potential problematic areas where concordance with standard guidelines is not yet be achieved. Continuous medical education, functional drug and therapeutic committees and regular drug utilization evaluation programs could help in accomplishing the milestone of rational medication use. Also use of procalcitonin (PCT) to improve diagnosis of bacterial infections and to guide antibiotic therapy in infected patients in intensive care unit, which have benefits to guide decisions about initiation and / or discontinuation of antibiotic therapy.