


1. Background
Poliomyelitis, commonly referred to simply as ‘polio’, is a debilitating infectious disease that may induce paralysis and neurological complications in humans. The causative agent of infection is polio virus (PV), a highly contagious enterovirus that is transmitted by the faecal-oral route. In the 19th and 20th centuries, polio was one of the most feared diseases in industrialized countries, causing ‘infantile paralysis’ of the legs, and less commonly, the head, neck and diaphragm, in several hundreds of thousands of children each year. However, after the introduction of effective vaccines in the 1950s and 1960s polio was all but eliminated as a public health problem [1]. There are two effective vaccines – one given by injection containing inactivated virus (IPV) and the other, more common, administered orally containing live, attenuated virus (OPV). By the 2000s, the worldwide threat of polio had abated as a result of continuing intensive immunization of children and adults against PV in multiple countries [2]. Additionally, an integrated system of surveillance for early detection of cases by screening for the three antigenically distinct serotypes of PV in a person’s faeces and in environmental samples has facilitated the identification of a threat in real time, thereby reducing the risk of onward dissemination [3].
Although the transcontinental control and prevention of polio is an undoubted public health success story, the final chapter is incomplete. Afghanistan, Pakistan and Nigeria remain regional hotspots where polio retains endemic status. In recent years the presence of polio in these three countries has posed a serious risk to human well being on a global scale due to potential exportation of the virus [4]. In order to embark upon these last frontiers in the battle against PV infectious disease monitoring organizations have recently increased their focus on the situation in both South-Central Asia and West Africa [5].
Following the Soviet Union intrusion for a nine year period from December 1979 the political situation in Afghanistan and the neigh bouring tribal belt of Pakistan has seen continued unrest and instability. Due to profound financial constraints that led to the neglect of healthcare systems under the control of successive governments anti-polio immunization coverage in the region has been woefully inadequate. Moreover, strong opposition by extremist groups that acted to cultiva tea sense of insecurity among healthcare staff has further compromised the efforts of immunization campaigns [6]. A lack of awareness of polio prevention among local people that has fueled controversies borne of scaremongering regarding the safety record of the administered vaccine is another compounding factor [7]. The geographical contiguity of Afghanistan and Pakistan presents an even greater obstacle due to the porous nature of their shared border which offers unrestricted cross-border movement for nomadic populations at many sites [8]. These collective circumstances have, to a large extent, facilitated the spread of polio infection and made the implementation of polio control measures extremely difficult. The situation in Nigeria manifests as a largely similar set of challenges [9]. No incidence of polio was reported for a period of three years from 2013 but the detection of three confirmed cases in late 2016 placed the country back on the list of endemic regions [10].
2. Action Plan Implementation
The renewed commitment of the World Health Assembly to polio eradication led, in 1988, to the launch by the World Health Organization (WHO) of the Global Polio Eradication Initiative, a program that has stepped up the rate and coverage of immunization over the last three decades [11]. Under this ongoing initiative Afghanistan and Pakistan are now considered as a single epidemiological block. In view of the need for improved management strategies, coordination and collaboration between the two countries has been enhanced [4]. The main polio reference laboratory in Islamabad, Pakistan’s capital city, is now used as the regional diagnosis centre for Afghanistan as well as for Pakistan [12]. In addition, cross-border surveillance has been strengthened and supervisory teams have been deployed to monitor people passing from one country to the other [4]. The WHO recommends polio vaccination for all residents and for visitors staying more than four weeks in the region [4].
Together with monitoring for acute flaccid paralysis, polio environmental surveillance, which is a key component of the polio surveillance system, has been focused in each of Afghanistan, Pakistan and Nigeria [12-14]. After the 2014 polio surge in Pakistan [15], environmental surveillance in the country received special attention[16]. Currently, Pakistan has a large network that comprises 53 active environmental sites [14], and the number of samples that are evaluated from each location is increasing annually in order to safeguard against any lapse in detection [14] (Figure 1). In West Africa, following the detection of new polio cases in Nigeria the bordering countries of Benin, Cameroon, Chad and Niger were also declared vulnerable and immunization has been recommended to combat with any possible influx of PV [4]. Historically, cross-border movement of people between Nigeria and neighboring nations has resulted in the bidirectional spread of the virus [13].

3. Action Plan Outcome
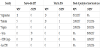
The enhanced focus on polio eradication in the form of the aforementioned measures has provided much needed impetus towards this ultimate public health objective. It is as a direct outcome of this bold action that after the 2014 surge (306 polio cases) in Pakistan, the toll of cases decreased dramatically to 54 in 2015 [15], and declined further to 20 in the subsequent year [16] (Table 1). Similarly, the number of cases in Afghanistan decreased from 28 in 2014, to 20 in 2015, and 13 in 2016 [15]. As of 6 December, in 2017 six cases have been reported from Afghanistan while three from Pakistan [17] (Table 1). The polio-centred public health initiative in Afghanistan has made steady progress whereas the outcome of a similar program in Pakistan is even more promising and commendable. A major factor contributing to the success achieved in Pakistan in a short time is attributed to an aggressive counter-terrorist operation launched by the Pakistan military in 2014 named ‘Zarb-e-Azb’. This resulted in bringing back miscreant-held areas under the writ of the national government, and now most of those regions have high priority status within the ongoing immunization program [16].
4. (Re)current Challenges
Despite this striking achievement, serious challenges remain along the path towards eradication. The issue of vaccine-derived outbreaks of infection is one such obstacle [4], even in non-endemic regions (Table 1). Increasingly, in order to prevent endemic transmission a monovalent OPV containing live, attenuated virus of a single serotype has been deployed to target areas where one serotype predominates. On rare occasions adverse events may occur when monovalent OPV viruses mutate to acquire the transmissibility and neurovirulence characteristics of wild type PV. This is of great concern because during defaecation some individuals may shed a mutated version of the administered OPV strain that regains the potential to paralyze healthy human beings. In such cases, vaccine-associated paralytic polio is clinically indistinguishable from disease manifestations caused by wild type PV. Hence, the risk of vaccine-derived PV circulating in environmental samples should be kept in mind and recommendations regarding the wisdom of maintaining stockpiles of monovalent OPV have been released recently [18].
The recent outbreak of circulating vaccine-derived polio virus (cVDPV) cases in Syria is a prime example of mutated OPV reversion-associated polio [19]. During 2017, as of 6 December, a total of 70 cVDPV cases have been reported in currently war-torn Syria, a country which has not had a case of indigenous wild type PV since 1999. DDR Congo and Lao are the two other polio nonendemic countries that have experienced incidences of cVDPV in recent years (for which the last reported case of indigenous wild type PV was in 2000 and 1996, respectively). A further drawback of the administered OPV relating to the error-prone replication of PV isits ability to recombine with picorna viruses, thereby posing a very rare but arguably unavoidable infection threat to vaccine recipients [20]. Due to both these issues outbreak response teams have turned to using IPV strategically to boost immunity. Additional vaccines are being prepositioned as part of ongoing contingency planning to ensure that, when the local security situation allows, programs are able to respond quickly in areas where cVDPV transmission is occurring [21].
In Nigeria, vaccine coverage in insurgent-invaded territories presents a significant challenge since all recent cases have been reported from miscreant-dominated areas [10]. Furthermore, insurgency is precipitating a crisis of internally displaced people, who are migrating to other regions for reasons of personal safety. The movement of refugees is an obstacle to immunization programs as some territories are inaccessible due to security reasons [13] (Figure 2). By December 2016, 39% of settlements in Borno state and 5% in Yobe state of Nigeria remained completely inaccessible, which represents a profound threat to the mission of global polio eradication [13].

Surveillance quality presents another major question. The authorities in Nigeria thought that they had eradicated wild polio virus serotype 1 (WPV1), but it turned out the virus had been circulating in Borno for many years without being detected because surveillance and vaccination could not reach those areas. Hence, zero detection from a selection of surveillance sampling sites does not necessarily mean that the virus has been eradicated. Rather, successful eradication of the virus can only be guaranteed by an extensively spread surveillance system with a strong environmental component. Therefore, entry to the currently inaccessible areas of Nigeria is imperative in order to be able to claim complete eradication [13].
Another serious hurdle to the control of polio is the act of noncompliance by parents who are not willing to cooperate with vaccination staff. In March 2017, 46,967 Pakistani parents refused to vaccinate their children against polio, including those belonging to the most educated socio-demographic sector [22]. Similarly, in 2014, on a single day of vaccination in Peshawar, close to the border with Afghanistan, 16,757 children did not receive the OPV due to parental prevention [7]. Incidents of refusal have also been reported from Afghanistan and Nigeria [23]. While the Government of Pakistan has taken stern action against defiant families, the reasons cited for refusal are multifactorial and therefore not straightforward to address to parental satisfaction. Many people in Afghanistan, Pakistan and Nigeria believe, incorrectly, that the vaccine contains non-halal ingredients [23,24], which are prohibited for Muslims to consume. Similarly, another misconception is that detrimental effects are caused by constituents of the vaccine which are included specifically to sterilize their children on the hidden agenda of the west [7,23,24]. The US Central Intelligence Agency-backed fake vaccination attempt in pursuit of militants, conducted in Abbottabad, Pakistan, compounded this trust deficit; this raised questions regarding the credibility of vaccination teams that consequently sabotaged the overall cause.
5. Future Solutions
Under the given circumstances, there is an urgent need to address the controversies associated with recent attempts to administer polio vaccination in the three countries discussed in which infection remains endemic. Mobilization of political leadership at all levels, security forces and adequate resources (domestic and international) are all needed for a high quality response. The safeguarding presence of the military and government-supported armed groups provides an opportunity to improve program accessibility for outbreak response, surveillance and routine immunization activities [13,16,25].
Delivery of community awareness programs at the level of villages and towns is imperative. The advocacy of expert medical scientists and high-ranking religious clerics is deemed to be effective in converting public opinion towards the pro-vaccination cause. The powerful influence of religion on the people of these regions is such that religious scholars are able to incite the general public. Among the major steps taken to nullify concerns about the non-halal content of the OPV is that it is now prepared in a Muslim country, Indonesia, under strict supervision for halal content [23].
Each of the currently polio-endemic countries is underdeveloped and the attitude of the general public is quite negatively reactive towards the virus, contrasting to the attitude widespread in developed nations where people are more proactive with regard to their health and wellbeing. Hence, the support of local communities is an important element of the plan to achieve polio eradication. This could be managed better by simultaneously educating people about the injurious effects of this public health menace and campaigning in favour of vaccination. Thus, by taking confidence-building measures and intensifying awareness programs, the ongoing hurdles to polio eradication could be effectively minimized. Only then will it be possible to reach every person in at-risk areas with the OPV, or its IPV alternative, to protect them against the disease and to increase herd immunity to the virus. Such an action plan would also further strengthen disease surveillance in order to ensure rapid detection and response wherever PV emerges.
6. Conclusion
Despite the unfortunate recent setback in Afghanistan and Pakistan due to a resurgence of polio cases and problems of accessibility to militant-held territories, the lack of cases reported in Nigeria since October 2016 is a clear indication of progress in the right direction towards global polio eradication. In order to achieve this triumph, currently inaccessible territories in all three countries demand urgent attention. Due to occasional cases of vaccine-derived polio in these and other nation in which public health systems are compromised, notably Syria at the present time, complete cessation may still take some time to be reached and confirmed.
In addition to the technical issues of vaccination coverage, the compounding factors of religious influences and vaccine safety concerns present serious challenges. The objective of addressing public apprehension through increased and improved awarenessbased schemes is imperative in order to achieve ultimate success. It is therefore apparent that a successful outcome of this final phase of the global polio eradication initiative is strongly linked to the winning of hearts and minds and the restoration of trust of the individuals in those communities affected.
Competing Interests
The authors declare that they have no competing interests.
Author Contributions
Both authors have made substantial contributions to the conception of the article, contributed significantly to writing the manuscript, revised it critically for important intellectual content, approved its final version and agreed to its submission.