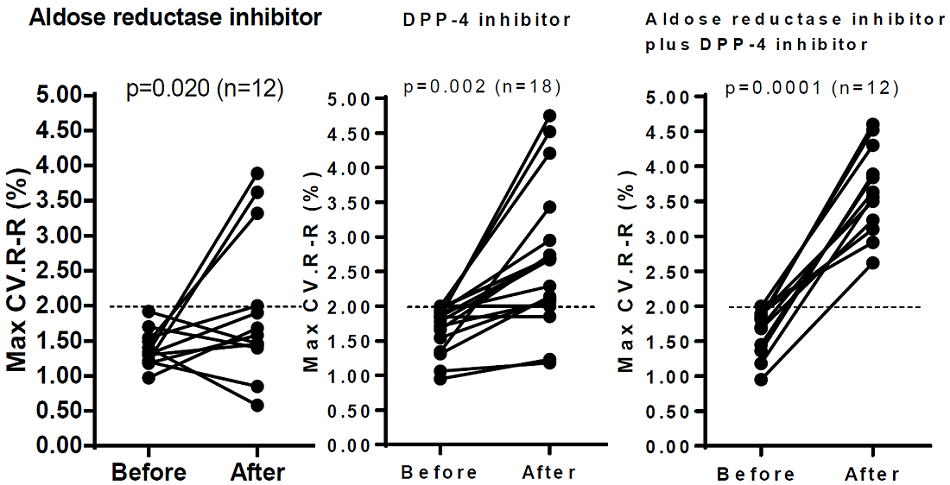
Figure 2: Changes in maximal CV. R-R with cardiac vagal neuropathy (CVN) before (group 1) and after treatment (group 2) with oral epalrestat 150 mg daily alone as aldose reductase inhibitor (ARI) in group A (n = 12) at the left side, before and after treatment with oral sitagliptin 50 mg daily alone, DPP-4 inhibitor as incretin-based therapy (IBT) in group B (n=18) at the center, and before and after treatment with the combination of ARI (oral epalrestat) and IBT (oral sitagliptin) with CVN in group C (n=12) at the right side. The broken line represents the low limit of the normal range in 100 consecutive maximal CV. R-R intervals (max CV.R-R) from usual breathing to deep breathing at rest for measurement on electrocardiography. CVN was defined as max CV. R-R less than 2.00% at all times during three measurements in diabetic patients. The CVN defined by max CV.R-R was represented as a kind of cardiac autonomic neuropathy (CAN).
A total of 42 patients with CVN and with type 2 diabetic patients (T2DM) were studied. They were divided into three groups (A, B, and C). Group A (n = 12) was treated with add-on oral epalrestat 150 mg daily alone as ARI, group B (n=18) was treated with add-on oral sitagliptin 50 mg daily alone, DPP-4 inhibitor as IBT, and group C (n= 12) with CVN despite treatment with oral epalrestat alone (n = 6) for 1 year in group A, oral sitagliptin alone (n = 5) for 1 year in group B and subcutaneously injection of GLP-1 receptor agonist (n =1) as IBT for 1 year was treated with add-on combined oral epalrestat and oral sitagliptin. The mean duration of each treatment was 1 year.
A total of 42 patients with CVN and with type 2 diabetic patients (T2DM) were studied. They were divided into three groups (A, B, and C). Group A (n = 12) was treated with add-on oral epalrestat 150 mg daily alone as ARI, group B (n=18) was treated with add-on oral sitagliptin 50 mg daily alone, DPP-4 inhibitor as IBT, and group C (n= 12) with CVN despite treatment with oral epalrestat alone (n = 6) for 1 year in group A, oral sitagliptin alone (n = 5) for 1 year in group B and subcutaneously injection of GLP-1 receptor agonist (n =1) as IBT for 1 year was treated with add-on combined oral epalrestat and oral sitagliptin. The mean duration of each treatment was 1 year.